

The thalamus and hypothalamus are complicated subcortical structures. While they both originate from the diencephalon, these two structures have starkly different roles within the central nervous system. The thalamus is a subcortical grey matter structure that acts as a major relay center between the cortex and other subcortical areas while the hypothalamus has many nuclei with various roles; hormone synthesis, temperature regulation, hunger/thirst, etc. The hypothalamic-pituitary axis is an important topic for introductory neuroanatomy courses but is considered low yield for in-service and board examinations. Because of this, the intricacies of this topic will not be covered in-depth in this chapter. The goal of this chapter is to review the complicated roles of the thalamus and associated pathology and briefly review hypothalamic nuclei.
Author: James Eaton, MD
Editor: Brian Hanrahan, MD, Steven Gangloff MD
Thalamus
- The thalamus is a collection of subcortical grey matter and part of the diencephalon (along with the hypothalamus) involved in relaying information between different functional regions of the CNS.
- It borders the dorsal part of the third ventricle and functions as part of the lateral wall of the ventricle.
Thalamic nuclei
- There are three main types of thalamic nuclei: relay, association, and nonspecific nuclei.
- Relay nuclei have very distinct inputs and outputs.
- Association nuclei receive a majority of their input from the cortex and project fibers to other cortical regions.
- Nonspecific nuclei broadly project to numerous cortical regions.
Relay nuclei
- Ventral posterior lateral (VPL) nucleus: Relay center for sensory information of the body. The output is to the postcentral (sensory) gyrus.
- Ventral posterior medial (VPM) nucleus: Relay center for sensory information of the face. The output is to the postcentral (sensory) gyrus.
- The VPM is also the relay center for taste.
- Lateral geniculate body/nucleus (LGN): Relay center for vision. Receives input from the retina with output to the primary visual cortex via optic radiations.
- Optic radiations from the lower visual field (upper retinal quadrants) travel through the temporal lobe (Meyer’s loop) and optic radiations from the upper visual field (lower retinal quadrants) pass through the parietal lobe.
- Medial geniculate body/nucleus (MGN): Relay center for hearing. Receives input from the inferior colliculi and projects to the primary auditory cortex.
- Ventral anterior (VA) nucleus: Conveys motor information from basal ganglia to the premotor cortex. It plays a role in the initiation of movement.
- Ventral lateral (VL) nucleus: Conveys motor information from both the cerebellum and basal ganglia to the primary motor cortex.

Association nuclei
- Mediodorsal nuclei (MDN): Receives input from the amygdala, subthalamic nucleus, and temporal lobe with output to the frontal cortex. It is involved in motivation and memory.
- Lesions to the mediodorsal nuclei can lead to amnesia, behavioral issues, and executive dysfunction.
- Anterior nucleus: Receives input from the mammillary bodies with output to the cingulate gyrus. It is important for limbic function and memory formation.
Nonspecific nuclei
- Reticular nucleus: Receives input from many cortical regions and projects directly onto other thalamic nuclei. It is the only thalamic nucleus that does not project to the cortex.
- It is thought to play a role in sleep-wake cycles.
Thalamic vascular supply
- There are four major vessels that supply the thalamus:
- Polar (tuberothalamic) artery
- Originates from the posterior communicating artery (PCOM).
- Anterior circulation strokes can present with anterior thalamic involvement due to the polar artery arising from the PCOM. All other thalamic strokes must arise from the posterior circulatory system.
- Supplies more anterior portion of the thalamus.
- Strokes affecting this artery lead to a wide range of neuropsychiatric changes.
- Originates from the posterior communicating artery (PCOM).
- Paramedian (thalamic-subthalamic) artery
- Originates from the P1 segment of the posterior cerebral artery (PCA).
- Supplies the dorsomedial nucleus.
- Infarction has a range of neuropsychiatric symptoms.
- Unilateral lesions can lead to language (dominant hemisphere) or visuospatial problems (non-dominant).
- Bilateral infarction can result in akinetic mutism. A top-of-the-basilar occlusion can commonly cause a bilateral infarction due to an anatomic variant known as the Artery of Percheron, where both paramedian arteries arise from a single pedicle on the P1 portion of PCA.
- Thalamogeniculate (inferolateral) artery
- Originates from the P2 segment of the posterior cerebral artery (PCA).
- The thalaMogeniculate artery supplies multiple nuclei including the Medial geniculate nucleus (MGN).
- Lesions lead to sensory loss, hemiparesis, and hemiataxia.
- Originates from the P2 segment of the posterior cerebral artery (PCA).
- Posterior choroidal artery
- Arises from the P2 segment of the posterior cerebral artery (PCA).
- Supplies the lateral geniculate nucleus (LGN) and pulvinar among other nuclei.
- Lesions lead to vision changes, variable sensory loss, weakness, and memory impairment.
- Polar (tuberothalamic) artery
Thalamic dysfunction
- Lesions to the thalamus can cause a wide range of symptoms and syndromes because there is much information being relayed through a relatively small area.
- Generally, lesions to a nucleus of the thalamus lead to dysfunction of that relay arc (e.g. lesion of the VPL leads to numbness of the contralateral body).
- Dejerine-Roussy Syndrome (thalamic pain syndrome)
- Contralateral hemisensory loss of all modalities followed by body pain.
- Akinetic mutism
- Can develop with thalamic lesions, presumably with the involvement of the mediodorsal nucleus (MDN).
- Akinetic mutism can also be seen in bilateral prefrontal lobe lesions or caudate lesions as well.
- Artery of Percheron Stroke
- This is a vascular anatomic variant where one artery supplies both paramedian regions of the thalamus.
- Clinically manifests with a decreased level of consciousness, hypersomnolence, aphasia/dysarthria, and oculomotor abnormalities.
Hypothalamus
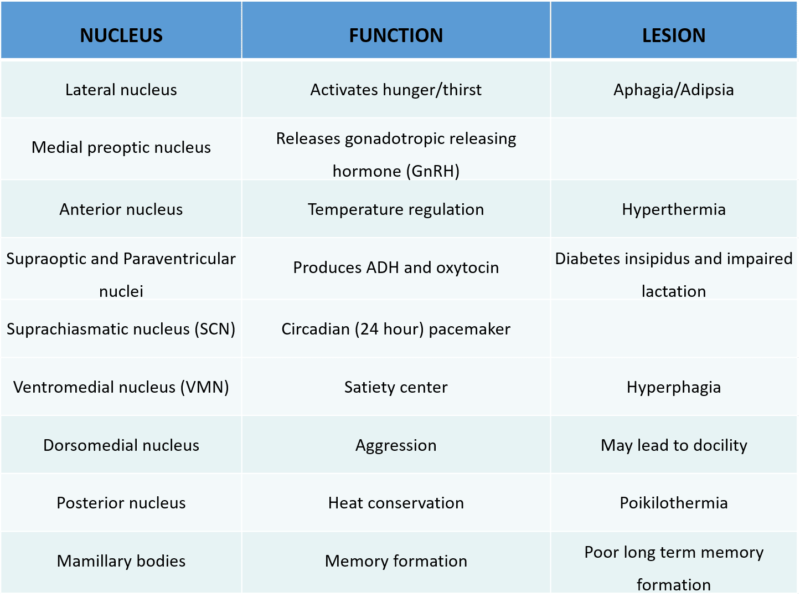
- The hypothalamus is considered to be the coordinating center of the endocrine system that helps to maintain homeostasis. It contains several nuclei with various functions (Table 1) including autonomic function, body temperature regulation, and water balance.
References
- Arend I.; Rafal R.; Ward R. (2008). “Spatial and temporal deficits are regionally dissociable in patients with pulvinar lesions”. Brain. 131 (8): 2140–2152.
- Diencephalon. In: Waxman SG. eds. Clinical Neuroanatomy, 28e New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com/content.aspx?bookid=1969§ionid=147036773.
- Mancall EL. Diencephalon. In: Gray’s Clinical Neuroanatomy: The Anatomic Basis for Clinical Neuroscience. Vol 1. Philadelphia, PA: Elsevier; 2011:261-278.
- Mtui E, Gruener G, Dockery P. Hypothalamus. In: Hypothalamus. 7th ed. Oxford, UK: Elsevier; 2016:253-259.
- Parent AD, Perkins E. The Hypothalamus. In: Fundamental Neuroscience for Basic and Clinical Applications. Vol 5. Philadelphia, PA: Elsevier; 2018:442-456.
- Schmahmann JD. Vascular syndromes of the thalamus. Stroke. 2003;34(9):2264-78.
- Swenson, Rand. “Chapter 10 – Thalamic Organization.” Chapter 10: The Thalamus, 2006, www.dartmouth.edu/~rswenson/NeuroSci/chapter_10.html. Accessed on 11/5/2019.
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
New here? Get started!
(Or, click here to learn about our institution/group pricing)1 Month Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
3 Month Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
1 Year Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
