

Congenital rubella
- A neuroinfectious disease that causes cataracts, congenital heart defects (PDA), deafness, microcephaly, and developmental delay. Less likely hepatosplenomegaly and jaundice.
- MRI with periventricular and cortical (especially basal ganglia) calcifications.
Congenital Toxoplasmosis
- Causes chorioretinitis (usually bilateral), macrocephaly (due to intrauterine hydrocephalus), seizures, developmental delay, jaundice, hepatosplenomegaly, thrombocytopenia, and purpuric rash.
- MRI with calcifications of the basal ganglia and corticomedullary junction.

Congenital Cytomegalovirus (CMV)
- Causes developmental delay, seizures, sensorineural deafness, hepatosplenomegaly, vision loss, microcephaly, and lissencephaly.
- This neuroinfectious disease is the leading cause of acquired hearing loss in childhood, and hearing loss may even occur in children who had an asymptomatic CMV infection at birth.
- Neuroimaging will show periventricular calcifications, profound cortical atrophy and ventriculomegaly. May also have associated anterior temporal cysts with white matter disease.

Neonatal herpes simplex
- Exposure to genital herpes through the birth canal.
- MRI with multifocal lesions, temporal lobe involvement, hemorrhages, and relative sparing of basal ganglia.
Congenital syphilis
- Presents at birth with mucoid or bloody nasal discharge (“snuffles”), long bone deformities, Hutchinson’s teeth, keratitis/blindness, and frontal bossing.
Congenital HIV/AIDS
- Symptom onset between 2 months and 5 years with a loss of milestones, failure of brain growth, ataxia, myoclonus +/- seizures, and spastic paresis.
- Pathology with multinucleated giant cells and calcific vasculopathy (see below).
- MRI with diffuse atrophy.

Bacterial Meningitis
Abundant gray-white exudate surrounding the brainstem and cerebellum secondary to pneumococcal meningitis.

Brain Abscess
Coronal section showing multiple well-circumscribed abscesses.
CNS abscess
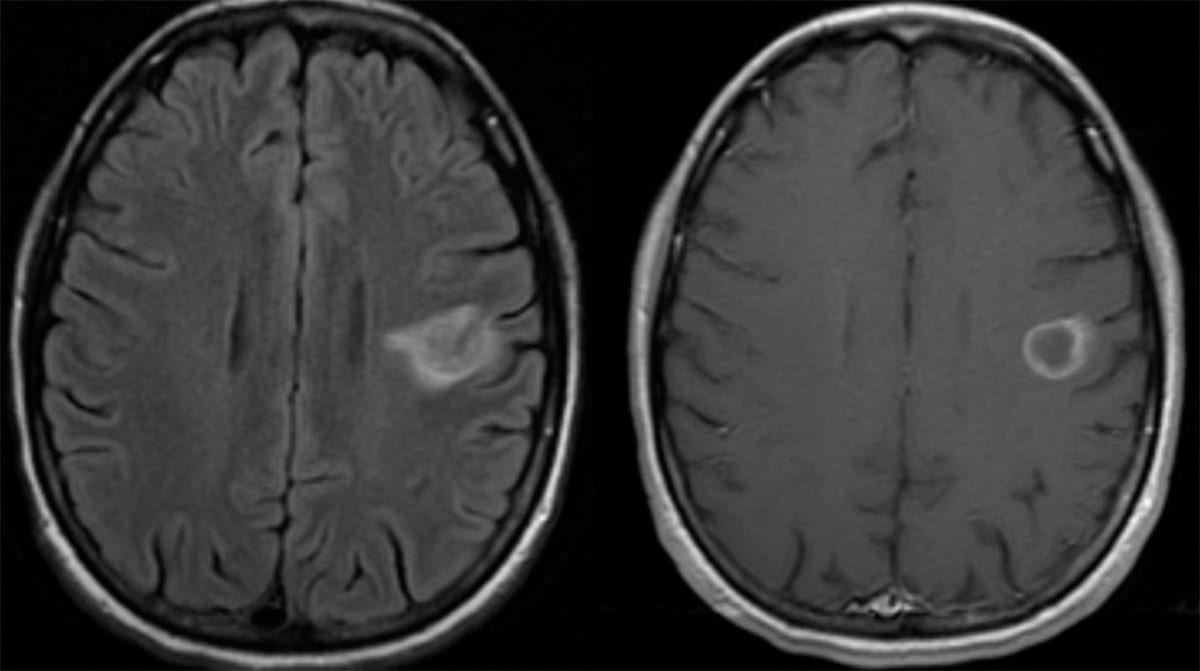
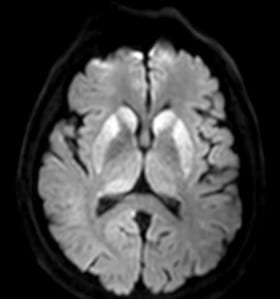
- It is high yield to be able to identify CNS abscess on MRI:
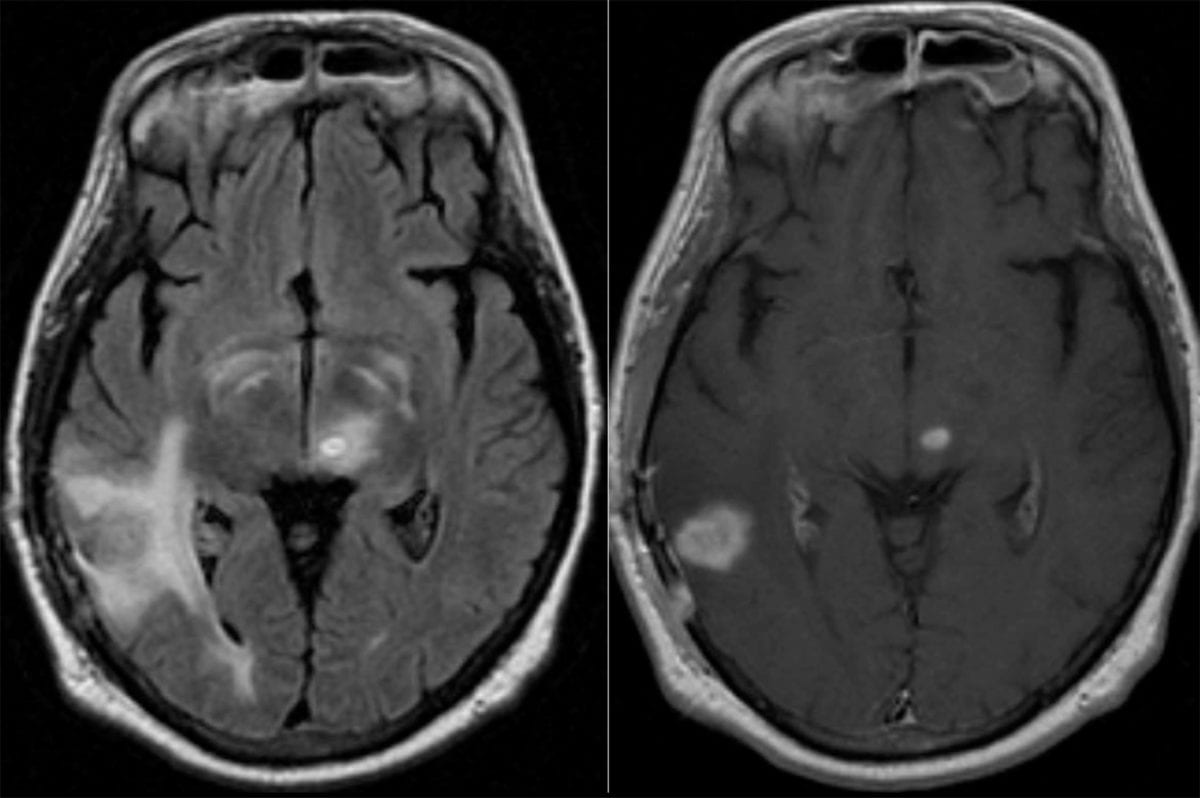
- An abscess will have internal restricted diffusion due to the presence of pus, with a smooth rim of enhancement and adjacent vasogenic edema.
- If multiple lesions are present, consider septic emboli.

- Citrobacter species, Serratia marcescens, Proteus, Pseudomonas, and Enterobacter are common causes.
- Ventriculitis is another possible complication of meningitis:
- On MRI, ventriculitis appears as fluid levels within the cortical sulci and within the posterior horns of the lateral ventricles with increased signal and on the T1-weighted postcontrast views with extensive enhancement of the ependyma.
- Lasting sequela of bacterial meningitis can include hearing loss, permanent motor deficits, learning disability, epilepsy, and/or hydrocephalus.
- The most common cause of brain abscess in immunocompetent patients is spread from nearby infection (otitis, mastoiditis > sinusitis).
- This accounts for 40-50% of cases.
- Hematogenous spread (such as from endocarditis) accounts for 30-40% of cases.
- Spread from distal infection (such as dental) is possible, but less common.
- Most significant predisposing factor for bacterial abscess in children is cyanotic congenital heart disease.
- Treatment:
- Empiric brain abscess antibiotic treatment includes a third-generation cephalosporin and metronidazole.
- Because >95% of brain abscesses are bacterial, and of those many are polymicrobial, broad-spectrum coverage is needed until a brain aspiration can confirm the pathogen.
- An exception is if endocarditis is already confirmed or highly suspicious, in which case IV nafcillin is often used.
- In addition to antibiotics, surgical drainage is a needed treatment.
- Glucocorticoids can be considered if the abscess has mass effect large enough to cause significant depression of mental status.
- Empiric brain abscess antibiotic treatment includes a third-generation cephalosporin and metronidazole.
Listeria monocytogenes
- Cover empirically in suspected meningitis patients who are >50 years old, <1 month old, immunocompromised, alcoholic, or pregnant.
- Treatment and empiric coverage: ampicillin.
- Classically associated with rhombencephalitis.
Bartonella henselae (Cat scratch disease)
- Infection typically presents as a mild self-limited febrile illness with adenopathy (often a single node in the arm, neck, or axilla).
- It can rarely cause cerebritis and clinical symptoms such as seizures, encephalopathy, and neuroretinitis.
- Neuroimaging often identifies demyelinating lesions.
- If neuroretinitis is present, there will be contrast enhancement at the junction of the globe and optic nerve on MRI and a “macular star” on ophthalmologic examination.
- Spread by cats, particularly feral kittens that live outdoors or in barns.
- CSF analysis is usually normal.
Borrelia burgdorferi (Lyme neuroborreliosis)
- Lyme disease presents acutely with local erythema migrans at the bite site with a viral-like syndrome. Progression to CNS Lyme (neuroborreliosis) will exhibit deficits in executive function, attention, organization, initiation, abstract concept formation, and verbal fluency.
- Spread by Ixodes tick.
- Diagnostic studies: Demonstration of intrathecal antibody production and cerebral spinal fluid (CSF) polymerase chain reaction (PCR) for the Borrelia spirochete.
- Pathology: Vasculitis, focal demyelination, and in the late stages, neuronal loss and gliosis.
- Imaging: Multifocal white matter lesions on MRI.
Tropheryma whipplei (Whipple disease)
- Gram-positive, non-acid-fast, periodic acid-Schiff (PAS) positive Bacillus.
- Presents with cognitive dysfunction, diarrhea, malabsorption, and weight loss.
- Occasionally can present with oculomasticatory myorhythmia (pathognomonic): continuous rhythmic eye movements with concurrent masticatory muscle contractions.
- PAS-positive macrophage inclusions are seen in intestinal biopsies.
Treponema pallidum (Syphilis)
- Five types (congenital, primary, secondary, latent, tertiary).
- Neurologic manifestations occur in tertiary syphilis, which occurs 3-25 years after infection onset and presents with tabes dorsalis (degeneration of the dorsal columns) or rarely paresis, and may demonstrate Argyll Robertson pupils (accommodates but does not constrict to light).
Mycobacterium leprae
- Tuberculoid leprosy
- Occurs in immunocompetent patients with limited disease.
- Presents with only a few plaques with well defined edges and enlarged, palpable nerves.
- Nerve biopsy would show granulomatous changes and few bacilli.
- Lepromatous leprosy
- Occurs in immunosuppressed patients
- Presents with widespread disease, with numerous skin lesions and a small fiber neuropathy involving ears and nose with decreased pinprick and reflexes.
- Always consider in patients from endemic counties.
Mycobacterium tuberculosis
- Presents with insidious meningitis with a preference toward the brainstem, namely the basal (interpeduncular) cistern, which consequently can cause cranial neuropathies (CN VI most commonly) and hydrocephalus.
- Also, 10% of cases involve the spine, and meningitis can progress to form tuberculoma.
- Tuberculous vasculopathy can cause bilateral MCA inflammation and strokes.
- Treatment: Isoniazid, rifampicin, pyrazinamide, and ethambutol
- Ethambutol has a 3% risk of causing optic neuritis. If seen clinically, discontinue ethambutol while continuing other aspects of treatment.

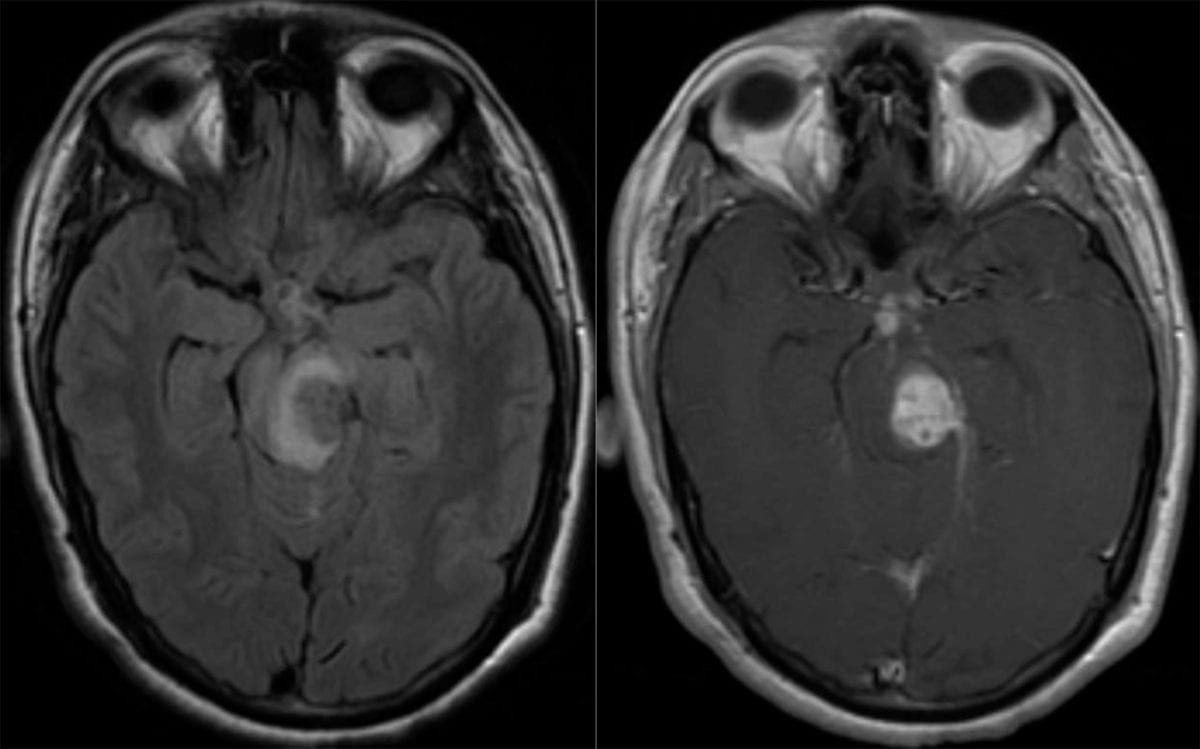
(Left) Axial FLAIR MRI shows an isodense lesion within the midbrain on left with surrounding edema. (Right) Axial T1 with contrast shows that the lesion is diffusely contrast-enhancing.
HSV
- Presents with personality changes, seizures, and meningitis symptoms (fever, headache, AMS).
- If the frontal lobe is involved there will be frontal release signs: grasp reflexes, echolalia, mutism, etc.
- If the temporal lobe is involved, the patient will have amnesia. Klüver-Bucy syndrome can be seen with bilateral involvement.
- CSF: Shows lymphocytic pleocytosis. HSV PCR is 100% specific and 95% sensitive but can be falsely negative in the first 72 hours of disease onset. Can also have elevated RBCs due to hemorrhagic changes in the temporal lobes.
- Treatment: IV acyclovir
- Pathology: Cowdry inclusions are intranuclear eosinophilic inclusions seen in viral infections, including HSV, but are not specific for any one virus.

HSV Encephalitis
High power microscope slide, H&E stain, showing intranuclear eosinophilic inclusions of nucleic acid called Cowdry bodies (arrows).

HSV Encephalitis
H&E stains showing Cowdry bodies (intranuclear eosinophilic inclusions of nucleic acid)(arrows).
- MRI: Inferior frontal lobe and medial temporal lobe involvement with edema, restricted diffusion, and contrast enhancement.
VZV
- May cause necrotizing retinitis, myelopathy or transverse myelitis, or large vessel cerebral vasculitis 1-2 weeks after a rash.
- The virus lays dormant in ganglion (typically in the thoracic cord) and utilizes axonal transport machinery to reach the skin surface.
- VZV is also capable of traveling centrally to the cord resulting in myelopathy.
- It can reactivate in the setting of immunosuppression.
- Usually, the skin will become erythematous prior to the rash appearing.
- If the skin of CN-V1 distribution is involved, keratitis can occur.
CMV
- As a neuroinfectious disease, CMV can cause transverse myelitis, radiculitis, cauda equina syndrome, or laryngeal nerve dysfunction in immunocompromised (AIDS) patients.
- Treatment: Ganciclovir and foscarnet.
EBV
- In immunocompetent hosts, it is often asymptomatic but can cause mononucleosis. Rarely, can cause a number of neurologic syndromes including facial nerve palsy, Guillain-Barre, aseptic meningitis, and varied other presentations.
- Identified in almost all cases of primary CNS lymphoma (PCNSL) in AIDS/immunocompromised patients. See our Tumors and Cysts Chapter for more information on PCNSL.
HHV6
- This neuroinfectious disease can cause post-transplant acute limbic encephalitis.
- A complication of bone marrow transplants.
- Presents as an amnestic syndrome typically within 60 days of a bone marrow transplant.
- The clinical picture usually progresses to encephalitis with seizures due to mesial temporal lobe involvement.
- Pathology: perivascular mononuclear cell inflammatory infiltrates, coupled with microglial clusters.
- Treatment: Foscarnet.
JC (John Cunningham) Virus
- Reactivation of latent JC virus is the pathophysiology of progressive multifocal leukoencephalopathy (PML).
- PML is usually a fatal opportunistic infection of the central nervous system within oligodendrocytes due to reactivation of latent JC polyomavirus infection.
- An immunocompromised state, such as those with HIV/AIDS or on disease-modifying agents such as natalizumab, can trigger JC virus reactivation.
- Patients who wish to start natalizumab for MS are required to have their JC titers checked before starting therapy.
- Treatment usually requires discontinuation of natalizumab or initiation of antiretrovirals if AIDS-related.
- Pathology: Intracellular oligendrocytic inclusions.
")
Progressive Multifocal Leukoencephalopathy (PML)
Axial T2 FLAIR showing hyperintensity of the left parietal region with involvement of the subcortical U-fibers. There is some mass effect present.
")
Progressive Multifocal Leukoencephalopathy (PML)
Axial FLAIR MRI with multiple areas of hyperintensity involving the medial temporal lobes, the right occipital lobe, and the splenium of the corpus callosum.
")
Progressive Multifocal Leukoencephalopathy (PML)
Left: Axial T1. Middle: T2 FLAIR. Right: T2 with contrast with extensive left parietal white matter hyperintensity. Enhancement, which is seen in this case, is atypical and more commonly seen in cases of PML induced by AIDS or natalizumab.
West Nile Virus (WNV)
- Transmitted by mosquitos
- Typically is asymptomatic but can cause meningitis, encephalitis, or myelitis with a particular affinity for anterior horn cells.
- Possible presentations include:
- Mental status changes
- Tremor secondary to a predilection for the basal ganglia and thalamus.
- Polio-like syndrome
- Cranial neuropathies
- No treatment is available, only supportive therapy.
Measles
- Can cause subacute sclerosing panencephalitis (SSPE), a rare form of chronic progressive brain inflammation.
- The course is asymptomatic for years, then progressive decline occurs first with behavior change, then intellectual problems and myoclonic seizures and blindness, then rigidity, then death.
- The EEG is nearly diagnostic in the myoclonic phase .

- Pathology: Intranuclear eosinophilic inclusions and demyelination.
- Diagnosis: Serum or CSF IgG.
HIV/AIDS
- Can present with mental and motor slowness, myelopathy, sensory neuropathy, and dementia. It can also cause HIV-associated vacuolar myelopathy affecting the dorsal columns.
- Pathology: Macrophages and multinucleated giant cells of infected cells in the perivascular spaces in white matter.

HIV Leukoencephalopathy
H&E stain showing gliotic white matter with two multinucleated cells, consistent with HIV encephalitis.

HIV Brain Biopsy
Brian biopsy with perivascular macrophages and multinucleate giant cells in white matter.
Rabies virus (lyssavirus)
- Rabies can be caused by a number of lyssaviruses.
- Commonly spread by bites from bats, raccoons, and skunks in the United States.
- Patients initially present with fever and altered mental status. Agitation and hydrophobia are seen in later stages.
- Pathology: Bullet-shaped eosinophilic cytoplasmic inclusions called Negri bodies.

Rabies cytoplasmic Inclusion
High-power view of the cerebellum showing a Purkinje cell with an eosinophilic inclusion called a Negri body.

Rabies
Low power microscope slide; H&E stained biopsy of cerebellum showing two eosinophilic Negri bodies within a Purkinje cell, characteristic of rabies.
Coccidioidomycosis
- Coccidioidomycosis (“valley fever”) is most commonly asymptomatic or purely pulmonary, but otherwise normal immunocompetent individuals may develop a disseminated disease and/or meningitis presenting with subacute unremitting headache.
- Endemic to the southwestern United States and northwestern Mexico.
- Pathology: individual spherules/endospores with a round and refractile wall.
- Diagnosis: CSF with pleocytosis, hypoglycorrhachia, and IgG cocci antibody. Fungal culture is low yield.
- Imaging: may show clusters of dilated Virchow-Robin spaces on T2-weighted MRI and multiple enhancing parenchymal and leptomeningeal nodules.
Histoplasmosis
- Located around the Ohio river valley.
- Budding yeast can be seen in the macrophage cytoplasm.
- It starts as a non-specific respiratory illness. It can disseminate to CNS in severe cases, causing chronic meningoencephalitis, focal parenchymal brain or spinal cord lesions, hydrocephalus, and even stroke from infected emboli.
Blastomycosis
- Usually a lung and sometimes skin/bone infection, but in immunocompromised patients can cause meningitis or brain abscess.
- Hyphae of Blastomyces have “broad-based buds”
- Treat with itraconazole.
Aspergillosis
- Commonly found in the upper respiratory tract of healthy individuals.
- This infection usually directly enters the CNS from the paranasal sinuses in diabetics or from immunosuppressed patients who have a systemic infection (i.e. leukemia, organ transplant, chronic steroid use).
- Cerebral infection occurs in 25-40% of those with disseminated aspergillosis.
- Fungal infection of the brain can lead to meningitis, multiple abscesses, and/or cerebral infarct due to obstruction of cerebral arteries by branched hyphae.
- Mycotic aneurysms can also occur, leading to intraparenchymal hemorrhage.
- Pathology:
- Vasoinvasive lesions appreciated by fungi branching at acute angles (hyphae) inside blood vessel walls are seen.
- Grey irregular necrotic masses can also occur.

Aspergillosis
Left: Silver stain showing fungal hyphae. Right: H&E stain showing fungal hyphae surrounding an artery.

Aspergillosis
Upper Left: High power microscope slide with silver stain for fungus highlighting hyphae. Center: Low power H&E stained microscope slide where a blood vessel is surrounded by inflammatory cells, with infiltration of the vessel wall by fungal hyphae.
- Imaging: Abscesses will present as a ring-enhancing lesion on contrasted imaging. T2-hyperintensities can represent regions of vasogenic edema from surrounding abscesses or cytotoxic edema from infarcted tissue.
Mucormycosis
- Rare but serious Rhizopus or Mucor species mold infection that can quickly travel to the brain through the sinuses.
- Presents with headache, proptosis, and facial numbness.
- Typically seen in poorly-controlled diabetic or immunocompromised (kidney transplant usually) patients.
- Hyphae grow in and around blood vessels, causing blood clots and necrosis.
- Treatment is surgical debridement of infected tissues and amphotericin B.
Cryptococcus
- This is the most common fungal meningitis, seen usually in AIDS patients (CD4 <200).
- Associated exposure with pigeons.
- Pathology: multiple bubbly cysts in the white matter, caudate, and putamen.

Cryptococcal Meningitis
Coronal section with numerous small intraparenchymal cysts located mostly in the superficial cortex with a few in deep gray matter. Cryptococcus predominantly involves the leptomeninges but tracks alongside the Virchow-Robin spaces into the parenchyma.

Cryptococcal Meningitis
Mucicarmine stain showing multiple red capsule-stained cryptococcus organisms (arrows).

Cryptococcal Meningitis
Capsule stain, low power (center) and high power (top left) with numerous small intraparenchymal cysts located mostly in the superficial cortex with a few in deep gray matter. Cryptococcus predominantly involves the leptomeninges but tracks alongside the Virchow-Robin spaces into the parenchyma.
Taenia solium (neurocysticercosis)
- Typically presents in Hispanic patients with partial-onset seizures and sometimes headaches and/or transient focal neurologic findings.
- This is the most common cause of acquired epilepsy in the developing world.
- Taenia solium can be found in undercooked pork or fecally contaminated water.
- Treatment: albendazole +/- dexamethasone to prevent inflammatory response to cyst death.
- Sometimes intraventricular cysts can lead to non-communicating hydrocephalus.
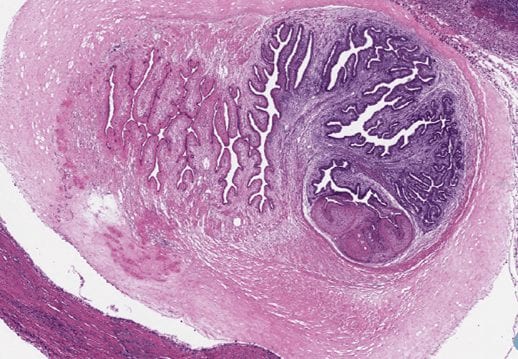
- Imaging: CT scan can show multiple calcified cysts. MRI brain with contrast can show ring-enhancing lesions with surrounding edema, most commonly at the gray-white junctions. Within these lesions, you will sometimes see the larval form of the Taenia sodium with an inverted scolex.
")
Cysticercosis (old)
Axial CT head showing multiple calcified lesions throughout the brain suggestive of a previous infection with cysticercosis.

Acute Cysticercosis
Left: Coronal T2-FLAIR MRI with a cystic lesion within the right frontal lobe with surrounding hyperintense signal indicating edema. Right: Axial T1-weighted MRI with contrast showing ring-enhancement.
- Taenia solium cysts can also be found in tissues other than the brain
Toxoplasma gondii (cerebral toxoplasmosis)
- This is an obligate intracellular parasite often found in cat feces.
- This neuroinfectious disease is the most common opportunistic infection in AIDS (CD4 < 100), as well as the most common focal mass lesion in AIDs.
- Treatment: Pyrimethamine (plus folate supplementation) and sulfadiazine.
- Pathology: microglial nodules with associated encysted bradyzoites and tachyzoites.

Toxoplasma Cysts
Brain biopsy showing toxoplasma cysts with encapsulated bradyzoites.

Toxoplasmosis
High-power view H&E stain showing abundant Toxoplasma tachyzoites (“free-floating” basophilic oval organisms) and bradyzoites (cysts containing protozoa).
- MRI: Lesions with prominent vasogenic edema, with nodular or ring enhancement on contrasted studies. Often involves the basal ganglia, thalamus, and corticomedullary junctions. It can be difficult to differentiate from lymphoma.
Plasmodium (malaria)
- “Cerebral malaria” can occur via sludging of infected erythrocytes in capillaries.
- Diagnosis: Giemsa-stained blood smear.
Naegleria fowleri
- The “brain-eating amoeba” that causes hemorrhagic meningoencephalitis.
- Rapidly growing and typically fatal amoeba infection that spreads from the nose to the brain through the sinuses.
- Seen after swimming in a warm freshwater pond/lake or using a neti pot with tap water.
- Prions are small misfolded and highly virulent proteins that alter the structure of other proteins nearby, thus acting like a spreading infection.
- Sporadic Creutzfeldt-Jakob disease (CJD)(85% of cases), familial CJD (10-15%), variant CJD, and fatal insomnia comprise the major prion disorders. Each of these disorders is characterized by rapidly progressive dementia.
- Once infected, the disease is irreversible and untreatable.
- Pathology: Spongiform changes in gray matter are the most specific histopathological finding. Neuronal loss and gliosis can also be present.
")
Spongiform Encephalopathy (CJD)
H&E stain showing many small round vacuoles consistent with spongiform encephalopathy.

Spongiform Encephalopathy
H&E stain showing many small round vacuoles consistent with spongiform encephalopathy.

Spongiform Encephalopathy
H&E stain showing many small round vacuoles consistent with spongiform encephalopathy.
- MRI findings include DWI hyperintensities of the cortex “cortical ribboning”, pulvinar, caudate, and/or putamen.
- Learn more about these prion disorders in the Dementia and Neurodegeneration Chapter.
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
