




Chiari Malformation
- Often congenital, these consist of herniation or atrophy of the rhombencephalon (hindbrain).
- Type I: Caudal displacement of the cerebellar tonsils between 3-5 mm into the upper cervical spinal canal.
- Associated with syringomyelia and Klippel-Feil anomaly but can also be asymptomatic and found incidentally.
- Type II: More extensive of an abnormality than a Type I malformation, a Type II malformation presents with the cerebellum, brainstem, and 4th ventricle extending beyond the foramen magnum.
- Most patients will also have a lumbosacral meningocele or myelomeningocele.
- Agenesis of the corpus callosum and abnormal cortical gyral patterns are other possible comorbid findings.

Arnold-Chiari Malformation
This midline sagittal section through the brain stem and cerebellum shows a downward displacement of the vermis and brain stem with beaking of the tectum.

Chiari 1 Malformation
Sagittal MRI showing the downward displacement of the cerebellum.

Chiari 1 Malformation
Sagittal MRI showing the downward displacement of the cerebellum.

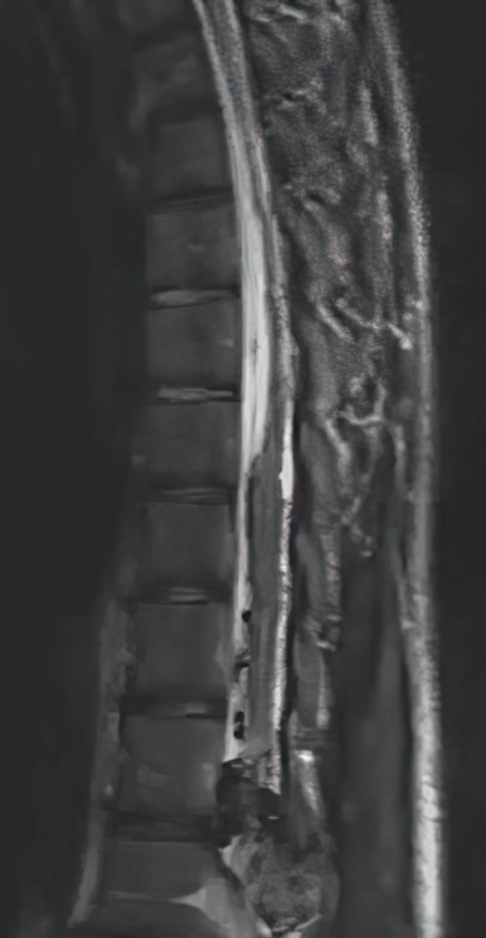
Chiari 1 Malformation with Holocord Syrinx
T2 FLAIR sequence, sagittal cut.
Klippel-Feil syndrome
- A congenital defect in which patients will have incomplete segmentation of the cervical spine with fusions of two or more vertebral bodies.
- Imaging: hypoplastic/absent intervertebral discs and continuous vertebral bodies.
Tethered cord syndrome
- MRI: downward extension of the conus, adhering within the sacrum.
- Traction of the conus medullaris leads to a progressive neurologic decline with weakness, sensory loss, and spasms in the legs, and loss of bowel/bladder function.
Spina Bifida
- Failure of proper closure of the neural tube resulting in caudal midline deformities.
- Risk factors include folate deficiency, valproic acid, genetic factors, a past child with spina bifida, obesity, and poorly-controlled diabetes.
- Types of spina bifida:
- Spina Bifida Occulta:
- The spinal sac closes but the vertebrae do not fully fuse.
- Signs are often minimal; a tuft of hair on the lower back, a birthmark, a sacral dimple, or a pilonidal cyst.
- Meningocele:
- Protrusion of meninges through the neural tube defect.
- Myelomeningocele:
- Both meninges and spinal cord protrude through the defect.
- The most severe type of spina bifida, which has significant associated neurological deficits from lower spine-related deficits (weakness, spasms, bowel-bladder dysfunction) to CNS issues (hydrocephalus, impaired cognitive development).
- Spina Bifida Occulta:

Lumbosacral Myelomeningocele
A flat open lesion consisting of vascular connective tissue and disorganized neural tissue.

Myelomeningocele
A large segment of dilated hydromyelic cord is seen within the cystic sac which is covered by skin.

Spina Bifida Diagram
Caudal Regression Syndrome
- Often (20% of cases) patients have mothers with diabetes.
- The lumbosacral cord is severely malformed, and may also have a tethered cord. The sacrum and limbs may be severely malformed, atrophic, or absent. Many patients do not survive. Those who do survive typically have normal cognitive development.
- Can be seen with the “VACTERL association”.
- Vertebral defects, Anal atresia, Cardiac defects, Tracheoesophageal fistula, Renal anomalies, and Limb abnormalities.
Dural AV fistula
- Can present with paraparesis and sphincter dysfunction, or occasionally only with radicular symptoms.
- Symptoms of myelopathy may be fluctuating and characteristically worsen with the Valsalva maneuver or exertion.
- Most commonly seen in the thoracic cord.
- Imaging:
- Longitudinally extensive central cord edema, with flow voids of dilated vessels on the surface of the spinal cord.
- Symptomatic fistulas should be treated with a spinal angiogram and intra-arterial repair or resection.
- Steroids should be avoided as they can worsen clinical outcomes.
Anterior spinal artery infarction
- The most common spinal cord infarct, it is often due to atherosclerosis or secondary to aortic surgery.
- Most likely to occur in the upper thoracic spinal cord (T1-T4), as this is the “watershed zone” for the spinal cord.
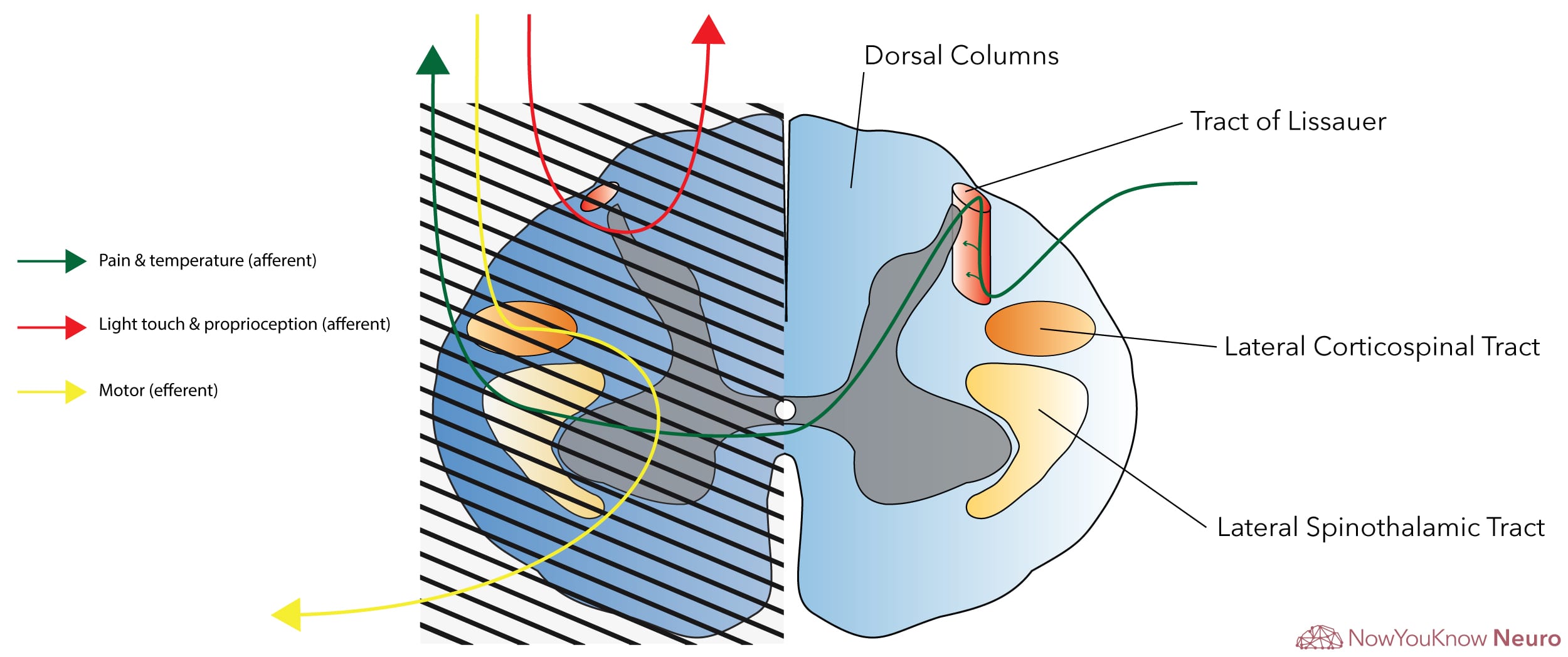
- Presents with anterior cord syndrome, which demonstrates acute onset weakness and loss of pain and temperature sensation below the lesion, while sparing the dorsal columns (light touch and proprioception). See diagram.
Central cord syndrome
- Classically characterized by predominant weakness in bilateral upper extremities that is greater than lower extremities. Can initially exhibit quadriplegia, but the lower extremity weakness often improves as edema goes down, while upper extremities remain weak.
- Also can present with “dissociated sensory loss,” where pain and temperature are diminished (compression of anterior white commissure) while proprioception and light touch perception are preserved. See diagram.
- Classically occurs after acute hyperextension injury in an elderly patient with preexisting spondylosis.
- A syrinx can also cause this syndrome, but a syrinx is typically slowly progressive and symptoms are often sensory-predominant.
- MRI reveals significant edema in the cord, most often in the cervical cord.
Conus medullaris syndrome
- Presents secondary to disc herniation, spinal stenosis, or a compressive mass at the conus medullaris.
- Causes hyperreflexia, upgoing plantar reflexes (upper motor neuron signs), saddle anesthesia, and sphincter dysfunction.
- High-dose methylprednisolone is used for traumatic cord compression, while high-dose dexamethasone is used for compression by tumors.
Cauda equina syndrome
- Can occur with disc herniation, spinal stenosis, or mass in the lumbosacral region causing compression on the spinal nerve roots, but not the cord.
- Presents with weakness, wasting, muscle fasciculations, hyporeflexia (lower motor neuron signs), and bowel/bladder/sexual dysfunction.
Brown-Sequard syndrome
- Cord hemisection caused by penetrating trauma such as a knife wound or gunshot wound.
- Presents with contralateral loss of pain and temperature sensation due to the involvement of the spinothalamic pathway and ipsilateral weakness and complete sensory loss at the level of the lesion, and weakness and loss of only proprioception and light touch sensation below the level of the lesion.
- The tract of Lissauer extends 1-3 vertebral segments. For this reason, the contralateral pain and temperature sensory loss is 1-3 spinal dermatomes lower than the level of the lesion.
- This occurs due to a hemisection of the cord through the anterior and posterior cord on one side. The crossed symptoms occur because the pain/temperature afferent pathway (spinothalamic tract) crosses within the cord while the fine touch/proprioception pathway (dorsal column-medial lemniscus (DCML) pathway) crosses in the medulla. See diagram to review.
Amyotrophic lateral sclerosis (ALS)
- Presents with both upper and lower motor neuron signs.
- In the spine, it is characterized by prominent alpha motor neuron atrophy in the anterior horn (similar to poliomyelitis) as well as the lateral corticospinal tracts. See diagram and the pathologic cross-section below.
- For more details on ALS, visit our Motor Neuron Disease chapter.

Transverse myelitis
- Diagnostic criteria include (1) bilateral sensorimotor and autonomic dysfunction, (2) a well-defined sensory level on examination, (3) an acute/subacute progression of symptoms (4 hours to 21 days), and (4) findings that suggest spinal cord inflammation (pleocytosis, elevated IgG index or MRI with an intramedullary spinal contrast-enhancing lesion).
- Differential diagnosis:
- Infectious:
- Most common infectious etiology is a viral infection (HSV/VZV/CMV/EBV, West Nile, etc.)
- HTLV and HIV can cause chronic myelitis.
- The most common parasitic cause worldwide is schistosomiasis
- Eggs are laid in the spinal cord. Treat with praziquantel.
- Bacterial etiologies include mycoplasma, syphilis, and Lyme disease.
- Most common infectious etiology is a viral infection (HSV/VZV/CMV/EBV, West Nile, etc.)
- Demyelinating disease:
- Neuromyelitis optica (NMO) and multiple sclerosis (MS) have a high association with transverse myelitis. See the Demyelinating Diseases chapter for more on these disorders.
- Those with aquaporin-4 antibodies are at high risk for disease relapse.
- other autoimmune diseases: SLE, Sjogren’s, mixed connective tissue disorder, scleroderma, sarcoidosis, and Behcet’s disease.
- Neuromyelitis optica (NMO) and multiple sclerosis (MS) have a high association with transverse myelitis. See the Demyelinating Diseases chapter for more on these disorders.
- Paraneoplastic syndrome:
- The most common antibody seen with paraneoplastic myelopathy is anti-Hu.
- Others include collapsin response-mediator protein 5 (CRMP-5) and GAD-65.
- Post-vaccination
- Infectious:
- Imaging:
- Spinal cord hyperintensity on T2-weighted MRI, which may enhance with gadolinium.
- Treatment with high-dose IV steroids is considered the first-line treatment.
Epidural abscess
- Presents with a typical triad of acute/subacute onset back pain, fever, and rapid progression of myelopathic deficits.
- Imaging: A fluid collection in the epidural space causing compression and displacement of the spinal cord.
- The typical MRI appearance is a loss of distinction between the endplates, disks, and adjacent vertebral bodies on T1-weighted views and increased T2- weighted signal. These areas show enhancement.
- Findings with high sensitivity for spinal infections include evidence of paraspinal or epidural inflammatory tissues, contrast enhancement of the disc, and hyperintensity on fluid-gradient T2-weighted views.
- Spinal infections rarely involve only one vertebral body and adjacent disc or only the epidural space.
- Most occur in the thoracolumbar region.
- Most common organism: Staphylococcus aureus.

Tabes dorsalis (syphilis)
- Seen in tertiary syphilis, this classically presents with dorsal column demyelination and degeneration, resulting in loss of light touch and proprioception (i.e. positive Romberg). See diagram.
- Numerous other manifestations are also common, including Argyll-Robertson pupils (accommodate but do not react), tabetic gait (locomotor ataxia), tabetic ocular crisis (pain syndrome), severe back pain, and psychosis or dementia.
- Diagnose with CSF VDRL.

Osteomyelitis
- Imaging: ring-enhancing lesion of the vertebra and not the disc.
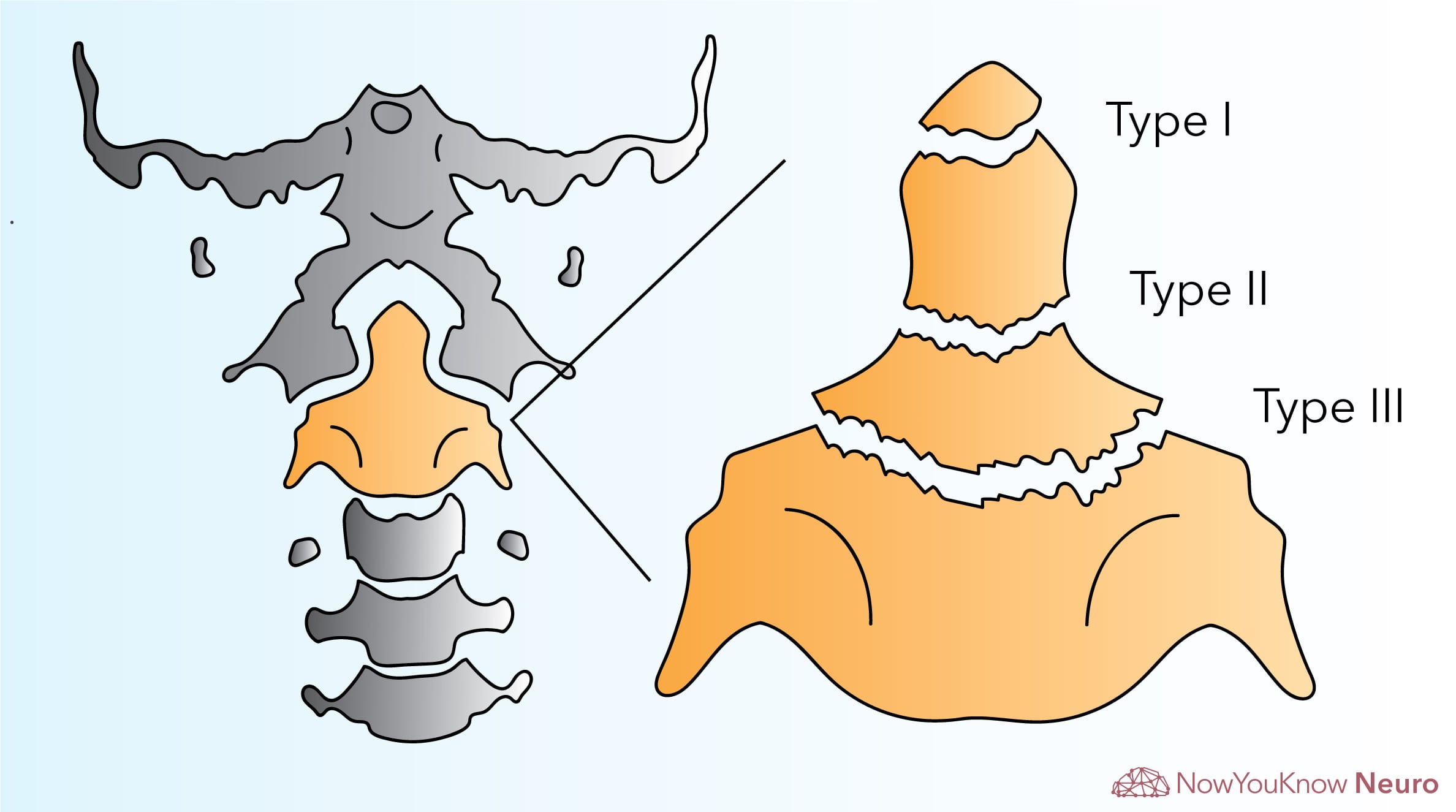
Odontoid fracture
- The odontoid, also known as the dens, is the body process from the C2 vertebra (axis), on which the C1 vertebra (atlas) pivots. The atlas and axis form the atlantoaxial segment of the spine.
- Patients with Down syndrome and rheumatoid arthritis are at a high risk of spinal cord injury due to atlantoaxial instability and subluxation.
- Fracture types:
- Type I: Considered a stable fracture, this type involves the tip of the dens, above the transverse ligament.
- Type II: Most common type, and considered unstable. This occurs at the base of the dens where it attaches to the C2 vertebral body.
- Type III: Usually unstable, this fracture type Involves the base of the dens as well as the facets lateral to the odontoid process. This type has the best prognosis for healing.
- For unstable fractures, spinal immobilization and urgent neurosurgical/orthopedic evaluation are indicated.
Burst fracture
- High axial stress causes compression and burst of vertebrae.
- Often from car collisions.
- Shards of bone from the injury can result in damage to the spinal cord.
Chance fracture
- Considered an unstable fracture, it is a fracture of the pedicle, vertebral body, and facet joints at multiple vertebral levels.
- Commonly occurs in the lower thoracic and upper lumbar regions.
- Due to hyperflexion of the spine, often seen in motor vehicle accidents in those wearing the lap belt without the shoulder belt.
Spondylolysis
- Also known as a fracture of the pars interarticularis of the spine.
- Typically asymptomatic but can progress to spondylotisthesis.
- Associated with repeated microtrauma leading to a stress fracture of the pars interarticularis, but could also be developmental.
- Imaging: bilateral defects of the pars interarticularis.
Spondylolisthesis
- Can be differentiated from spondylolysis due to the separation of the fractured pars interarticularis bone, leading to movement of the vertebrae in relation to the rest of the spine.
- Imaging: displacement of a vertebra relative to its adjacent ones.
- Can occur from hyperextension injuries, such car accidents or contact sport injuries. Can also be seen with “hangman’s fractures” where the C2 vertebrae is displaced anteriorly relative to the C3 vertebrae.
Disc herniation
- Imaging: Most often you will see an anterior mass lesion that is continuous with the nucleus pulposus. Lesions will be isointense to the vertebral disc in all MRI sequences.
- Most commonly this compresses nerve roots causing lower motor neuron signs, but can also compress the cord causing upper motor neuron signs.

L4-L5 Disc Herniation

L4-L5 Disc Herniation

S1 Disc Herniation
Spinal stenosis
- Imaging: Narrowing of the central canal between ligaments and osteophytes causing impingement and signal change in the cord.
- Symptoms: Pain in the posterior part of the thighs and calve after walking or standing. Symptoms often resolve with sitting and resting.
Ankylosing spondylitis
- Ankylosing spondylitis is a chronic, inflammatory disease of the axial spine.
- Calcification and fusion of vertebral ligaments and fusion of the facet joints lead to a decreased axial range of motion.
- Radiographic imaging can show a “bamboo spine” sign secondary to significant vertebral fusion.
Chordoma
- Arises from the remnants of the notochord.
- A slow-growing, primary bone tumor that can be found in the clivus or, more commonly, in the sacrum/coccygeal region.
- Imaging will show a destructive bony lesion extending into adjacent structures.
- Typically seen in adults (40-60 years of age).
- Treatment involves en-bloc resection of the tumor followed by radiation therapy due to the high recurrence rate.

T1-weighted MRI, sagittal cut showing a destructive lesion arising from the clivus

Lumbar spine MRI showing a destructive sacrococcygeal lesion suggestive of chordoma
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
