

Cranial nerves are a basic neuroanatomy topic that is heavily tested early in clinical training. As one transitions to later phases of their career (internship and residency), the focus moves away from the intricacies of neuroanatomy and more to the associated pathology.
Authors: Brian Hanrahan MD, Steven Gangloff MD
The Basics
- Cranial nerves are identified by either their complete name (Olfactory nerve) or by their Roman numeral (Cranial nerve I, CN 1). These terms are used interchangeably throughout this chapter.
- There are 12 sets of cranial nerves that carry sensory and/or motor fibers.
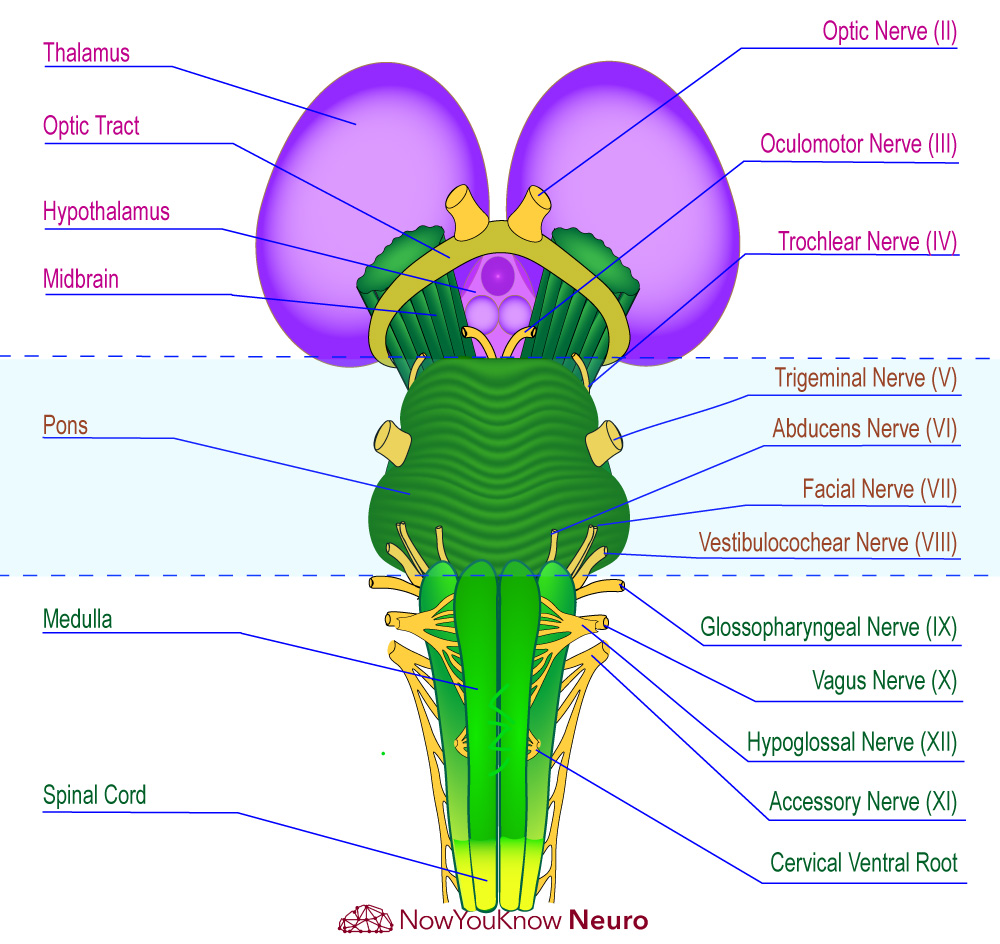
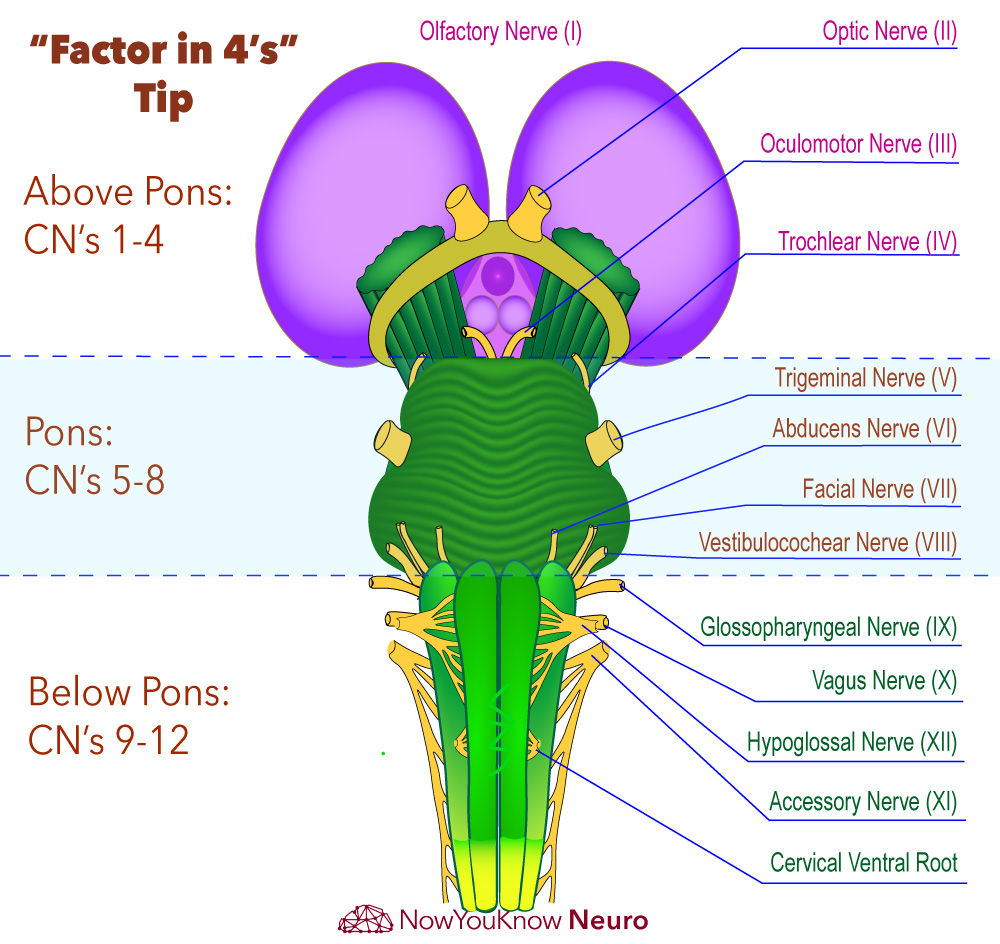
- Cranial nerves I and II are the only two that do not exit the brain at the level of the brainstem.
- Cranial nerves III and IV exit at the level of the midbrain.
- Cranial nerves V, VI, VII, and VIII exit at the level of the pons.
- Cranial nerves IX, X, XI, and XII exit at the level of the medulla.
- Cranial nerves IV, VI, XI, and XII are pure motor nerves.
- Cranial nerves III, IV, and VI control eye movements and pupillary constriction.
- Cranial nerves I, II, and VIII are pure sensory nerves.
- Cranial nerves V, VII, IX, and X are mixed nerves.
- Cranial nerves III, VII, IX, and X carry parasympathetic fibers.
Cranial Nerves & Brainstem Diagram
Move the Slider to Practice!


Cranial Nerve I (Olfactory Nerve)
- Sensory: Responsible for the sense of smell.
- Nerve fibers traverse the skull through the cribriform plate where neurons synapse directly with the cortex with no relay through the thalamus.
- Pathology:
- Head trauma can cause damage to the olfactory nerve as it travels through the cribriform plate leading to anosmia.
- Olfactory groove meningiomas can also present with anosmia.
Cranial Nerve II (Optic Nerve)
- Sensory: Responsible for visual sensory input.
Cranial Nerve III (Oculomotor Nerve)
- Motor: Innervates numerous extraocular muscles: superior rectus, inferior rectus, medial rectus, and inferior oblique as well as the levator palpebrae.
- It also provides parasympathetic innervation to the pupillary constrictor and ciliary muscles (the efferent limb of the pupillary reflex).
- Pathology:
- An oculomotor nerve palsy can present with a combination of four possible clinical features; ptosis, ocular deviation, mydriasis, and diplopia.
- Ptosis occurs secondary to the loss of innervation of the levator palpebrae muscle.
- Ocular deviation (down and out) and diplopia occur due to unopposed action of the lateral rectus and superior oblique muscles.
- Mydriasis occurs due to damage to the parasympathetic fibers which supply the pupillary constrictor and ciliary muscles.
- Possible etiologies include trauma, diabetes, hypertension, subarachnoid hemorrhage, and compression from a posterior communicating aneurysm or uncal herniation.
- An oculomotor nerve palsy can present with a combination of four possible clinical features; ptosis, ocular deviation, mydriasis, and diplopia.
Cranial Nerve IV (Trochlear Nerve)
- Motor: Innervates the superior oblique muscle, which is responsible for internal rotation and depression of the eye.
- Pathology:
- Exits the brainstem dorsally
- Of the cranial nerves, CN IV has the longest intracranial course.
- Patients will complain of diplopia and difficulty descending stairs.
- On exam, patients will often tilt their head away from (contralateral to) the affected side to compensate for extorsion of the ipsilateral eye.
Cranial Nerve V (Trigeminal Nerve)
- The trigeminal nerve exits the brainstem at the level of the pons and trifurcates into three branches (ophthalmic (V1), maxillary (V2), and mandibular (V3) before exiting the skull.
- The ophthalmic division (V1) traverses the skull through the Superior orbital fissure.
- The maxillary division (V2) traverses the skull through the foramen Rotundum.
- The mandibular division (V3) traverses the skull through the foramen Ovale.
- Mnemonic: “Standing Room Only”
- Sensory: Responsible for all modalities of sensation of the face.
- The ophthalmic division (V1) of the trigeminal nerve innervates the scalp, forehead, upper eyelid, conjunctiva and cornea of the eye, and the meninges.
- The maxillary division (V2) supplies sensory innervation to the lower eyelid and cheek, upper lip, upper teeth, gums, the nasal mucosa, the palate, and the roof of the pharynx.
- The mandibular division (V3) provides sensation to the cheek, the external auditory meatus, the tympanic membrane, the lower teeth and gums, the anterior 2/3 of the tongue, the lower lip, and the chin.
- Motor: Innervates the muscles of mastication (masseter, temporalis, medial, and lateral pterygoids), tensor veli palati, anterior belly of the digastric, mylohyoid, and tensor tympani.
- The motor fibers of the trigeminal nerve exit the skull via the foramen ovale along with the other mandibular division (V3) fibers.
- Pathology:
- Associated symptoms with a trigeminal lesion include impaired facial sensation and impaired hearing of the ipsilateral ear secondary to damage to the tensor tympani muscle.
- These symptoms can be seen in Wallenberg’s syndrome which is due to damage to the lateral medulla from a posterior inferior cerebellar artery (PICA) ischemic stroke.
- Trigeminal neuralgia (Tic douloureux):
- Compression of the trigeminal nerve can lead to trigeminal neuralgia which presents with intermittent, severe sharp/stabbing-like paroxysms of the face. Episodes usually occur for only a few seconds at a time.
- The sensory examination of the face is typically normal.
- Common triggers for pain include brushing teeth, washing the face, and strong winds hitting the face.
- Carbamazepine is the first-line therapy.
- Associated symptoms with a trigeminal lesion include impaired facial sensation and impaired hearing of the ipsilateral ear secondary to damage to the tensor tympani muscle.
Cranial Nerve VI (Abducens Nerve)
- Motor: Innervates the lateral rectus muscle, which is responsible for lateral deviation (abduction) of the eye.
- Pathology:
- A lesion to the abducens nerve will lead to dysfunction of the lateral rectus muscle and the unopposed action of the left medial rectus muscle, causing the affected eye to be turned nasally.
Cranial Nerve VII (Facial Nerve)
- Motor: Innervates the stapedius, buccinator, posterior belly of the digastric, and the muscles of facial expression.
- Sensory: Responsible for lacrimation, salivation (submandibular and sublingual), taste from the anterior 2/3rds of the tongue, and sensation of the external ear.
- Pathology:
- Bell’s palsy is a facial nerve mononeuropathy that presents with acute unilateral weakness of upper and lower facial muscles secondary to a non-specific viral infection.
- This is the most common cause of facial nerve paralysis.
- The second most common cause of facial nerve paralysis is herpes simplex virus (HSV) reactivation.
- Treatment: Prednisone to reduce inflammation +/- valacyclovir for severe cases (House-Brackmann Grade IV or higher, identified by an inability to fully close the eye).
- Ramsay Hunt Syndrome:
- Also called geniculate neuralgia or nervus intermedius neuralgia.
- Typically described as paroxysms of severe pain deep in the ear. It can also present with hearing loss, bitter taste, tinnitus, and vertigo secondary to viral spread to the vestibulocochlear nerve.
- On examination, a vesicular rash is usually present in the external acoustic meatus and lateral tongue.
- Pathophysiology: The herpes zoster virus (VZV) lies latent in the geniculate ganglia after initial infection. Reactivation of the virus causes inflammation of the nerve within the narrow stylomastoid foramen, leading to damage to the nerve.
- Herpes zoster virus (VZV) can also cause facial nerve mononeuropathy.
- It is more often seen in immunocompromised patients.
- Bell’s palsy is a facial nerve mononeuropathy that presents with acute unilateral weakness of upper and lower facial muscles secondary to a non-specific viral infection.
- Weakness of the stapedius muscle causes hyperacusis because the bone is unable to cover the oval window to protect it from low vibratory tones.
- Lyme disease can cause unilateral or bilateral facial nerve palsies as well as multiple cranial neuropathies.
- Infection-related facial mononeuropathies often make a complete or near-complete recovery and rarely recur.
- Non-infectious causes of facial nerve mononeuropathy include sarcoidosis, diabetes, Sjögren’s syndrome, and amyloidosis.
Cranial Nerve VIII (Vestibulocochlear Nerve)
- CN VIII exits the cranium via the internal acoustic meatus.
- Sensory: Responsible for auditory sensory input (cochlear nerve) and maintaining equilibrium (vestibular nerve).
- Auditory pathway: Spiral ganglion → superior olivary nucleus and trapezoid body → lateral lemniscus → inferior colliculus → medial geniculate nucleus → auditory cortex.
- mnemonic: The internal acoustic meatus is SSLIM.
- Auditory pathway: Spiral ganglion → superior olivary nucleus and trapezoid body → lateral lemniscus → inferior colliculus → medial geniculate nucleus → auditory cortex.
- Pathology:
- Benign Paroxysmal Positional Vertigo (BPPV):
- Within the inner ear, there are three canals that are responsible for maintaining balance with fast head movements. If calcium carbonate crystals (canaliths) within the canal(s) are dislodged, they can provide a false sensation of movement.
- Canaliths are also known as otoliths
- Patients present with nausea and positional vertigo.
- Diagnosis can be readily made with the Dix-Hallpike test which will provoke upbeat and torsional nystagmus.
- The Epley maneuver is often curative and can be simply performed in the clinic visit with a very high success rate (>90%).
- Within the inner ear, there are three canals that are responsible for maintaining balance with fast head movements. If calcium carbonate crystals (canaliths) within the canal(s) are dislodged, they can provide a false sensation of movement.
- Benign Paroxysmal Positional Vertigo (BPPV):
- Unilateral peripheral vestibular dysfunction leads to the patient falling towards the affected ear.
Cranial Nerve IX (Glossopharyngeal Nerve)
- Motor: Innervates the stylopharyngeus.
- Sensory: Responsible for taste sensation of the posterior 1/3 of the tongue, salivation (parotid gland), and autonomic monitoring via chemo- and baroreceptors of the carotid body and sinus.
- The baroreceptor reflex is essential in regulating responses to blood pressure changes through changes in sympathetic tone. When the blood pressure drops, it is detected by baroreceptors that cause an increase in sympathetic drive to increase heart rate, in an attempt to preserve perfusion pressure in the brain. The central locations of baroreceptors are in the aortic arch and the carotid sinus.
- Aortic arch baroreceptor information travels to the nucleus tractus solitarius, and then to the ventrolateral medulla, via the aortic nerve (Nerve of Cyon), which combines with the vagus nerve (CN X).
- Carotid sinus baroreceptor information, however, primarily reaches these same nuclei via the glossopharyngeal nerve (CN IX).
- The baroreceptor reflex is essential in regulating responses to blood pressure changes through changes in sympathetic tone. When the blood pressure drops, it is detected by baroreceptors that cause an increase in sympathetic drive to increase heart rate, in an attempt to preserve perfusion pressure in the brain. The central locations of baroreceptors are in the aortic arch and the carotid sinus.
- Pathology:
- Glossopharyngeal Neuralgia
- Presents with intense and paroxysmal pain of the ear and tonsillar fossa which can be triggered by coughing or swallowing.
- Syncope can occur due to inappropriate carotid sinus/body sensory fiber activation.
- Glossopharyngeal Neuralgia
CN IV: superior oblique.
CN VI: lateral rectus.CN V: anterior belly of digastric and tensor tympani.
CN VII: posterior belly of digastric & stapedius.
CN IX: stylopharyngeus.
Cranial Nerve X (Vagus Nerve)
- Motor: Innervates the muscles of the pharynx and larynx, and only one tongue muscle: palatoglossus.
- Sensory: Responsible for taste sensation of the epiglottis as well as visceral sensation of the heart, lungs, and gastrointestinal tract.
- The vagus nerve derives its fibers from the nucleus ambiguus, the dorsal motor nucleus, and the nucleus solitarius.
- The nucleus ambiguus supplies branchial motor fibers that travel in the vagus nerve to the muscles of the pharynx and larynx.
- The dorsal motor nucleus provides parasympathetic innervation to the heart, lungs, and digestive tract.
- The nucleus solitarius is responsible for taste and visceral sensory information from the heart, lungs, and gastrointestinal tract.
- Pathology:
- The recurrent laryngeal nerve is a pure motor branch of the vagus nerve which innervates the laryngeal muscles. Damage to this nerve by trauma, thyroid surgery, or compressive neoplasm can lead to hoarseness, dysphagia, and hypophonia.
Cranial Nerve XI (Spinal Accessory Nerve)
- Motor: Innervates the sternocleidomastoid and trapezius muscles.
Cranial Nerve XII (Hypoglossal Nerve)
- Motor: Innervates the extrinsic muscles of the tongue (genioglossus, hyoglossus, and styloglossus).
- The only “glossus” it does not innervate is palatoglossus, which is innervated by CN X.
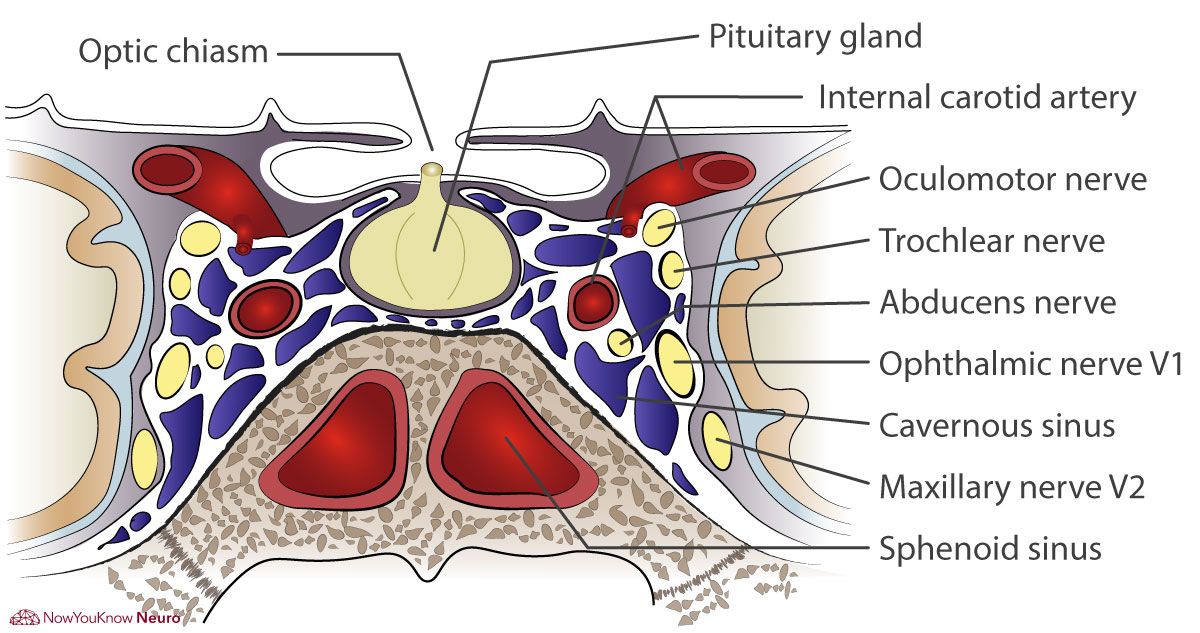
Cavernous sinus
- Several cranial nerves travel through the cavernous sinus. This includes CN III, IV, VI, V1 & 2 (the ophthalmic and maxillary branches of V), and sympathetic nerve fibers.
- Pathology:
- CN VI is the closest to the internal carotid artery and is most likely to be damaged with carotid dissection.
- Cavernous Sinus Syndrome:
- Presents with papilledema, proptosis, and painful ophthalmoplegia.
- Proptosis is secondary to occlusion of ophthalmic veins.
- A cavernous sinus thrombosis is a common cause, often secondary to infection from orbital cellulitis or sinusitis.
- Diabetes is a risk factor.
- Presents with papilledema, proptosis, and painful ophthalmoplegia.
Cavernous Sinus Diagram
Move the Slider to Practice!

Cranial Nerve and Skull Foramen
Cranial nerves exit through the skull via various foramen and canals. It is very important to be able to identify all of these foramina on gross anatomy and/or neuroimaging, know what structures pass through them, and appreciate the associated possible pathologies. This is very high yield.
High-yield foramina and associated structures
- Cribiform plate: Olfactory Nerve (CN I)
- Optic canal: Optic nerve (CN II)
- Superior orbital fissure: All of the nerves of extraocular movements (oculomotor nerve (CN III), trochlear nerve (CN IV), abducens nerve (CN VI)) as well as the ophthalmic branch (V1) of the trigeminal nerve (CN V).
- Foramen Rotundum: Maxillary branch (V2) of the trigeminal nerve (CN V)
- Foramen Ovale: Mandibular branch (V3) of the trigeminal nerve (CN V)
- Mnemonic: “Standing Room Only” for V 1/2/3.
- Internal auditory meatus: Facial nerve (CN VII) and vestibulocochlear nerve (CN VIII)
- After the facial nerve exits the skull via the internal auditory meatus, it enters the narrow stylomastoid foramen. The facial nerve within the stylomastoid foramen can be a point of inflammation in Bell’s palsy. It also contains the stylomastoid artery.
- Jugular foramen: Glossopharyngeal nerve (CN IX), vagus nerve (CN X), and spinal accessory nerve (CN XI)
- Hypoglossal canal: Hypoglossal nerve (CN XII)
- Foramen magnum: The ascending fibers of the spinal accessory nerve (CN XI) enter the skull via the foramen magnum before exiting the skull via the jugular foramen.
- Also contains the medulla and vertebral arteries.
- Foramen lacerum: Contains the greater petrosal and deep petrosal nerves.
- The internal carotid artery runs along, but not technically through, this foramen.
- Foramen spinosum: Middle meningeal artery/vein and meningeal branch V3.

Cranial Nerve Reflexes
Corneal Reflex
- The corneal reflex is a protective blink response.
- The afferent limb is the ophthalmic division of the trigeminal nerve (V1).
- The efferent limb is the facial nerve (VII) which innervates the orbicularis oculi muscle.
Pupillary Reflex
- The pupillary reflex is the constriction of both eyes in response to light, even if only a single eye is exposed to the light.
- The afferent limb is the optic nerve (CN II).
- Optic nerve fibers synapse on the pretectal nucleus. Pretectal neurons will then synapse on bilateral Edinger-Westphal nuclei.
- The efferent limb is the oculomotor nerve (CN III)
- The Edinger-Westphal nuclei are responsible for sending preganglionic parasympathetic fibers to the ciliary ganglia.
- Preganglionic fibers travel via the oculomotor nerve (CN III) and synapse at the ciliary ganglion. Cell bodies within the ciliary ganglion then carry postganglionic parasympathetic fibers to the sphincter muscle of the iris and the ciliary muscles.
- Both the ipsilateral (direct reflex) and contralateral (consensual reflex) pupillary constriction can give insight into the integrity of the oculomotor nerves.
- Pathology:
- Any lesion to the optic nerve (I.e. optic neuritis) can cause loss of both the direct and consensual reflex.
- Lesion to the ipsilateral oculomotor nerve and/or Edinger-Westphal nucleus leads to loss of the direct pupillary reflex.
- Lesion to the contralateral oculomotor nerve and/or Edinger-Westphal nucleus leads to loss of the consensual pupillary reflex.
Baroreceptor Reflexes
- The baroreceptor reflex helps to regulate blood pressure by detecting changes via a baroreceptor located in the carotid sinus and aortic arch. Increased pressures marked by these receptors produce slower heart rates and drops in blood pressure. A decrease in blood pressure produces an increase in sympathetic tone and a decrease in parasympathetic tone.
- The afferent limb is the glossopharyngeal nerve for the carotid sinus and the vagus nerve for the aortic arch.
- The efferent limb is the vagus nerve (CN X).
Gag Reflex
- The afferent limb is the glossopharyngeal nerve (CN IX).
- The efferent limb is the vagus nerve (CN X).
Important Nuclei
Nucleus tractus solitarius
- Both taste (rostral nucleus) and baroreceptor (caudal nucleus) information.
- CN VII: taste to anterior 2/3 tongue
- CN IX: taste to posterior 1/3 tongue, and baroreceptor from carotid sinus.
- CN X: taste to the pharynx, and baroreceptor from the aortic arch.
- Information travels to the VPM of the thalamus.
Nucleus ambiguus
- Corticobulbar input is bilateral.
- Motor fibers to pharynx/larynx/palate via CN IX, X, and XI.
References
- Beal M, Hauser SL. Trigeminal Neuralgia, Bell’s Palsy, and Other Cranial Nerve Disorders. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 20e New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com/content.aspx?bookid=2129§ionid=192532818. Accessed November 04, 2019.
- Cranial Nerves and Pathways. In: Waxman SG. eds. Clinical Neuroanatomy, 28e New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com/content.aspx?bookid=1969§ionid=147036627. Accessed November 04, 2019.
- Diseases of the Cranial Nerves. In: Ropper AH, Samuels MA, Klein JP, Prasad S. eds. Adams and Victor’s Principles of Neurology, 11e New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com/content.aspx?bookid=1477§ionid=215146778. Accessed November 04, 2019.
- Epley, J. M. (1992). The Canalith Repositioning Procedure: For Treatment of Benign Paroxysmal Positional Vertigo. Otolaryngology–Head and Neck Surgery, 107(3), 399–404. https://doi.org/10.1177/019459989210700310
1 Month Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
3 Month Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
1 Year Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
New here? Get started!
(Or, click here to learn about our institution/group pricing)1 Month Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
3 Month Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
1 Year Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
