

On average, 30-40% of patients admitted to the Epilepsy Monitoring Unit are diagnosed with a non-epileptic paroxysm. While a large majority of these cases are psychogenic non-epileptic attacks (PNEA), there is a long list of paroxysms that can be misdiagnosed as epilepsy. Below is a breakdown of various high-yield paroxysms by age.
Author: Brian Hanrahan, MD
Newborn period
Benign neonatal sleep myoclonus
- Clinical features of benign sleep myoclonus are repetitive, high-frequency myoclonic jerks of the limbs. Myoclonus can be generalized or involve a single limb.
- It typically appears soon after falling asleep and disappears with arousal.
- Symptoms resolve by 4-6 months of age.
- Treatment is not needed. Anti-epileptic drugs may make movements worse.
Hyperekplexia
- Presents as a sudden, exaggerated startle response followed by prolonged rigidity and apnea. Episodes are often triggered by an unexpected auditory or tactile stimuli.
- Several genes have been related to the disease but the most common is a glycine receptor alpha-1 subunit (GLRA1) gene mutation.
- Secondary hyperekplexia can also be seen secondary to a brain injury.
- In severe cases, clonazepam can be used for treatment.
- Phenobarbital may be considered as a second line agent.
Jitteriness
- The most common paroxysm appreciated in the neonatal period.
- Movements are best described as involuntary, rhythmic, oscillatory tremors.
- Can be triggered by touching the affected limb and suppressed with flexing the affected limb.
- Risk factors for jitteriness include prematurity, intracranial hemorrhage, sepsis, maternal substance abuse, and hypothermia. They can also be benign in the first few days of life.
Infancy and Childhood
Benign paroxysmal vertigo (BPV)
- BPV is felt to be a migraine equivalent seen in children younger than 6 years of age.
- Episodes consist of dizziness, nausea/vomiting, and gait disturbance, lasting less than 5 minutes in duration.
Reminder
Benign paroxysmal vertigo (BPV) is different than benign paroxysmal positional vertigo (BPPV)
Benign paroxysmal torticollis
- Likely BPV, benign paroxysmal torticollis is classed as a migraine equivalent.
- Episodes consist of head-turning, vomiting, and pallor of the face. These paroxysms can last between a few hours to a few days.
- The first symptoms occur between 2-8 months of age and resolve by 5 years of age.
Breath-holding spells
- Presents between the ages of 6 months to 5 years.
- Breath-holding spells come in two forms; pallid and cyanotic
- Cyanotic breath-holding spells:
- 65-85% of breath-holding spells are cyanotic.
- Episodes occur when excessive crying by a child causes hypopnea/apnea. This, in turn, leads to cyanosis, hypoxia, and loss of consciousness.
- Pallid breath-holding spells:
- Cases occur secondary to fearful stimuli, which provokes sudden bradycardia, increased vagal tone, and loss of consciousness.
- Iron deficiency anemia is a common comorbidity.
Stereotypies
- Described as hand wringing, clapping, or flapping of the arms.
- Typically seen in patients with intellectual disability (i.e. Fragile X syndrome, autism, etc.)
Alternating hemiplegia of childhood
- Presents with recurrent episodes of paralysis, lasting several minutes to days, involving one limb, multiple limbs, or even both sides of the body
- Onset is before 18 months of age
- Symptoms resolve with sleeping, but can return upon awakening.
- Associated with ATP1A3 mutations.
Parasomnias (See sleep disorders chapter)
Tics (See movement disorders chapter)
Migraine (See headache chapter)
Adolescence/Adulthood
Syncope
- The most common paroxysmal event in adulthood.
- Patients with syncopal events often have some myoclonic jerks during loss of consciousness and little to no post-ictal confusion.
- Vasovagal syncope
- Accounts for 85% of syncopal events under 40 years of age
- Triggered by a precipitant such as pain, emotions, cough, and micturition.
- Prodromal symptoms of lightheadedness, dizziness, diaphoresis, tunnel vision, and nausea often occur.
- Cardiovascular syncope
- Results from bradyarrhythmia or tachyarrhythmia leading to a drop of blood pressure
- Typically seen in patients with underlying heart disease.
- Patients often had little to no prodrome before loss of consciousness.
- Orthostatic syncope
- Most common cause of syncope in the elderly.
- Occurs secondary to the inability of the autonomic nervous system to adapt to the demands of stress (i.e. position change)
- Defective vasoconstriction and excessive pooling of venous blood leads to cerebral hypoperfusion
- Risk factors include diabetes, neurodegenerative disease, dehydration, and the use of vasodilators or diuretics.
- Diagnosis can be made with tilt table testing.
- A positive tilt table test occurs when there are syncopal/presyncopal syndromes along with bradycardia or hypotension.
Psychogenic non-epileptic events
- Accounts for 30% of patients who are admitted to the epilepsy monitoring unit.
- Comorbid psychiatric disease and a history of abuse are common in patients with PNEA.
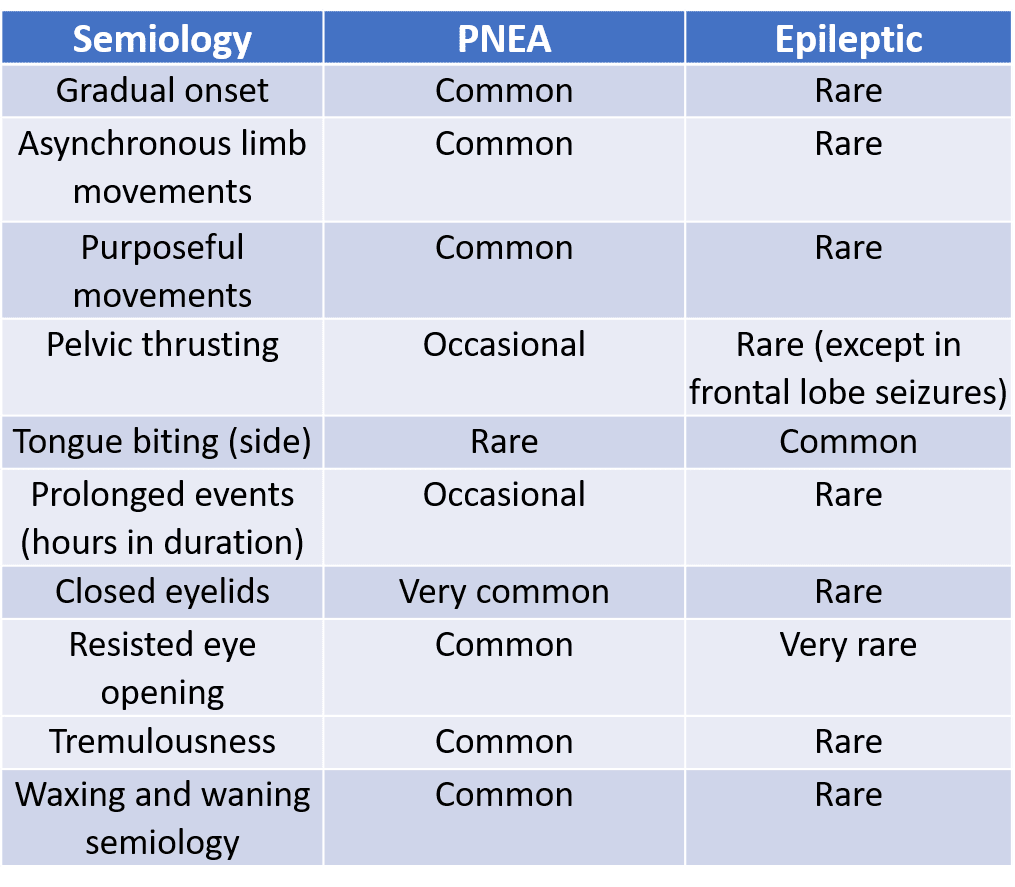
- Common clinical symptoms that differentiate PNEA from epileptic seizures include eye closure, pelvis thrusting, asynchronous limb movements, and/or generalized shaking with retained awareness (see table below).
- A definitive diagnosis can only be made with an epilepsy monitoring unit stay where the event in question is captured and there is no abnormal cortical activity appreciated on electrocorticography.
- Treatment
- Cognitive-behavioral therapy.
- Antiepileptic drugs have no benefit in the management of PNEA.
- Pharmacotherapy can be used to treat comorbid psychiatric disease.
Table 1: Ictal semiology for PNEA vs. Epileptic seizures
Parasomnias (See sleep disorders chapter)
Tics (See movement disorders chapter)
Migraine (See headache chapter)
References
- Ammirati, Fabrizio, et al. “Electroencephalographic Correlates of Vasovagal Syncope Induced by Head-Up Tilt Testing.” Stroke, vol. 29, no. 11, 1998, pp. 2347–2351., doi:10.1161/01.str.29.11.2347.
- Bowman ES. “Psychodynamics and Psychiatric Diagnoses of Pseudoseizure Subjects.” American Journal of Psychiatry, vol. 153, no. 1, 1996, pp. 57–63., doi:10.1176/ajp.153.1.57.
- Galanopoulou, A. S. and F. A. Lado (2004). “CLASSIFICATION, PATHOPHYSIOLOGY, CAUSES, DIFFERENTIAL DIAGNOSIS OF PAROXYSMAL EVENTS.” 10(4): 11-41.
- Goldman RD. Breath-holding spells in infants. Can Fam Physician. 2015;61(2):149–150.
- King RA, Nelson LB, Wagner RS. Spasmus Nutans: A Benign Clinical Entity? Arch Ophthalmol. 1986;104(10):1501–1504. doi:10.1001/archopht.1986.01
- Nechay A, Ross LM, Stephenson JB, O’Regan M. Gratification disorder (“infantile masturbation”): a review. Arch Dis Child. 2004;89(3):225–226. doi:10.1136/adc.2003.032102
- Tatlı, Burak, and Serhat Güler. “Non epileptic paroxysmal events in childhood.” Turk pediatri arsivi vol. 52,2 59-65. 1 Jun. 2017, doi:10.5152/TurkPediatriArs.2017.4588
Loading table of contents...
Loading table of contents...
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
New here? Get started!
(Or, click here to learn about our institution/group pricing)1 Month Plan
Full Access Subscription
$142.49
$
94
99
1 Month -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
3 Month Plan
Full Access Subscription
$224.98
$
144
97
3 Months -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
1 Year Plan
Full Access Subscription
$538.47
$
338
98
1 Year -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
Popular
