

Language disorders beautifully demonstrate the intersection of neuroanatomy and the physical exam. An understanding of both is imperative to being a successful neurologist.
Author: Brian Hanrahan MD, Steven Gangloff MD
Disorders of articulation
- Dysarthria: impairment in pronunciation with errors that are consistent and predictable secondary to disturbances in muscle function, whether it be due to weakness, paralysis, or incoordination.
- Apraxia of speech: Articulatory errors are variable and effect the prosody of speech.
Types of dysarthria
Flaccid (bulbar palsy)
- Occurs with lower motor neuron disease/neuromuscular junction disease:
- Commonly seen in patients with bulbar predominant myasthenia gravis.
- Presents with hypernasal speech and imprecise consonants.
Spastic (pseudobulbar palsy)
- Secondary to bilateral lesion in corticobulbar (upper motor neuron (UMN)) tracts.
- Occurs in patients with primary lateral sclerosis (PLS), amyotrophic lateral sclerosis (ALS), progressive supranuclear palsy (PSP), stroke, and other disorders.
- Presents with a harsh, hypernasal, mono-pitched voice, dysarthria, dysphagia, facial and tongue weakness, and emotional lability.
- Jaw jerk reflex will be positive and fasciculations are absent (because UMN affected).
Ataxic
- Presents due to the inaccuracy of muscle movements from cerebellar dysfunction.
- Seen with acute alcohol intoxication but can be irreversible with chronic use.
- Speech can be described as imprecise and scanning, with inconsistent errors in articulation.
Hypokinetic
- Seen in patients with Parkinson’s disease.
- The speech is described as monotonous and hypophonic.
Hyperkinetic
- Seen with dystonia and chorea which cause hypotonia and incoordination.
Note
Patients with ALS who have both upper and lower motor neuron disease can present with either a bulbar or pseudobulbar palsy.
Disorders of language
- Language dysfunction can present with variable degrees of comprehension or expression, with variable awareness of their deficit.
- Language has 6 characteristics:
- Fluency, comprehension, repetition, reading, writing, and naming.
Aphasic syndromes
Global aphasia
- Presents with complete loss of language fluency, comprehension, and repetition.
- Occurs due to large dominant hemisphere lesions such as a complete MCA ischemic stroke.
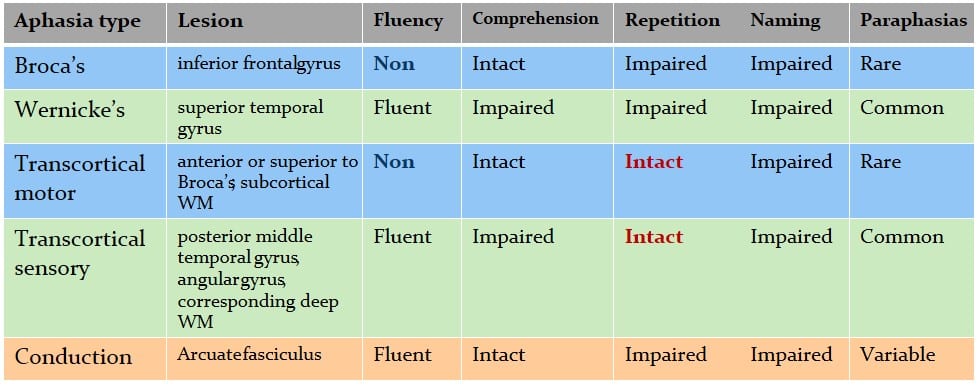
Broca’s aphasia
- Presents with poor fluency and retained comprehension.
- Patients will speak in short phrases that contain important content words.
- Mild cases may present with just agrammatic speech.
- Agrammatism is the inability to speak in a grammatically correct fashion with the simplified formation of sentences.
- Severe cases can lead to a complete loss of articulation.
- Patients are usually frustrated by their language disorders.
- Repetition is impaired.
- Lesion: Posterior inferior frontal lobe .
- Face and arm weakness usually occurs due to the proximity of the precentral gyrus to Broca’s area.
Wernicke’s aphasia
- Also called sensory or fluent aphasia.
- Presents with varying degrees of comprehension impairment with intact fluency.
- Mild cases present with paraphasic and semantic errors in their speech.
- Paraphasic errors: The swapping of sounds or syllables.
- If paraphasic word errors are so significant that the target word is unclear, it is called a neologism.
- Semantic errors; The substitution of related words.
- Paraphasic errors: The swapping of sounds or syllables.
- More significant presentations will have fluent, completely unintelligible speech, and impaired comprehension of written and spoken words.
- Patients are often unaware of their deficits.
- Like Broca’s aphasia, Wernicke’s aphasia also presents with impaired repetition.
- Lesion: Superior temporal gyrus
Transcortical motor aphasia
- Presents similarly to Broca’s aphasia but has retained repetition.
- Can be seen secondary to border zone infarcts involving the dominant frontal lobe, including the supplementary motor area.
Transcortical sensory aphasia
- Presents similarly to Wernicke’s aphasia but has retained repetition.
- Can be seen secondary to border zone infarcts involving the posterior temporal lobe and temporal-parietal-occipital junction.
Fast Fact
Transcortical aphasias are much less common than Wernicke's or Broca's aphasias. Despite their similar deficits, transcortical aphasias can be easily differentiated from their more common counterparts based on whether repetition is intact or not.
Conduction aphasia
- Presents with an isolated deficit in repetition, while other domains of language are intact.
- Occurs due to damage to the arcuate fasciculus.
Aphasia’s and their characteristics
What you need to know:
If interested in objectively evaluating someone's language deficits, a Boston Naming Test can be performed.
Anomic aphasia
- Presents with difficulty in word retrieval (especially nouns and verbs) but normal fluency and comprehension.
- Occurs secondary to a lesion in the dominant hemisphere, but it is not well localized.
Pure Word deafness
- Unable to repeat or comprehend spoken language but can still communicate via writing.
Aphemia (apraxia of speech)
- Non-fluent spoken language with preservation of comprehension and written communication.
Expressive aprosody
- Also known as amelodia or affective motor aprosodia.
- Not a true “aphasic syndrome” but occurs secondary to damage to the non-dominant posterior inferior frontal lobe, analogous to the non-dominant Broca’s area.
- Presents with the inability to produce melodic expression and loss of nonverbal expression.
Figure: Aphasia syndrome diagnosis algorithm

Thalamic aphasia
- Presents similarly to transcortical motor and sensory aphasias (retained repetition but impaired fluency and comprehension).
- May also present with behavioral changes and amnesia.
Progressive language disorders
Primary progressive aphasias (PPA)
- Exam: Predominant language impairment characterized by word-finding trouble, and difficulty with naming and comprehension. Initially, there are no other significant cognitive or behavioral problems but dysfunction of other domains develops over time.
- Pathology: Neurodegeneration of the language-dominant hemisphere.
- Three main variants: Nonfluent PPA, Semantic dementia, and Logopenic progressive aphasia.
Nonfluent PPA
- Subtype of frontotemporal dementia (FTD)
- Presents with at least agrammatism or effortful, halting speech with inconsistent speech-sound errors.
- The characteristic that distinguishes the nonfluent variant from other forms of PPA is the articulatory difficulty.
- Atrophy on MRI or SPECT hypometabolism of the dominant posterior frontal and insular regions can be seen.
Semantic dementia
- Subtype of frontotemporal dementia (FTD)
- Presents with impaired confrontation naming and impaired single-word comprehension. This leads to difficulty in understanding nouns and recognizing objects. Spontaneous speech is fluent and repetition and grammar are unaffected.
- Word-finding difficulty can be the earliest symptom.
- Concurrent symptoms: Visual agnosia and prosopagnosia.
- Atrophy on MRI or SPECT hypometabolism of the dominant anterior temporal lobe can be seen.
- If prosopagnosia is also present, hypometabolism will also be seen in the non-dominant anterior temporal lobe.
Logopenic progressive aphasia (LPA)
- Subtype of Alzheimer’s disease
- Presents with impaired single-word retrieval and repetition with errors in spontaneous speech and naming. Single-word comprehension, object knowledge, motor speech, and grammar are spared.
- Atrophy on MRI or SPECT hypometabolism of the dominant temporal-parietal region can be seen.
Primary Progressive Aphasias (PPA)
| Logopenic PPA | Semantic PPA | Nonfluent/agrammatic PPA | |
| Grammar | Normal | Normal | Impaired |
| Comprehension | Normal | Impaired single word comprehension | impaired comprehension of grammatically complex sentences |
| Naming | Impaired | Impaired | Normal |
| Object Knowledge | Normal | Impaired | Normal |
| Paraphasias | Present | Sometimes present | Present |
| Speech Rate | Moderately reduced | normal | Significantly reduced |
References
- Cauquil-Michon, Cécile, et al. “Borderzone Strokes and Transcortical Aphasia.” Current Neurology and Neuroscience Reports, vol. 11, no. 6, 2011, pp. 570–577., doi:10.1007/s11910-011-0221-z.
- Darley, Frederic L., et al. “Differential Diagnostic Patterns of Dysarthria.” Journal of Speech and Hearing Research, vol. 12, no. 2, 1969, pp. 246–269., doi:10.1044/jshr.1202.246.
- Dronkers, N.f., and J.v. Baldo. “Language: Aphasia.” Encyclopedia of Neuroscience, 2009, pp. 343–348., doi:10.1016/b978-008045046-9.01876-3.
- Gorno-Tempini, Maria Luisa, et al. “Cognition and Anatomy in Three Variants of Primary Progressive Aphasia.” Annals of Neurology, vol. 55, no. 3, 2004, pp. 335–346., doi:10.1002/ana.10825.
- Jonas, Saran. “The Thalamus and Aphasia, Including Transcortical Aphasia: A Review.” Journal of Communication Disorders, vol. 15, no. 1, 1982, pp. 31–41., doi:10.1016/0021-9924(82)90042-9.
- Nadeau, Stephen E., and Bruce Crosson. “Subcortical Aphasia.” Brain and Language, vol. 58, no. 3, 1997, pp. 355–402., doi:10.1006/brln.1997.1707.
- Ottomeyer, Caroline, et al. “Aphemia: an Isolated Disorder of Speech Associated with an Ischemic Lesion of the Left Precentral Gyrus.” Journal of Neurology, vol. 256, no. 7, Jan. 2009, pp. 1166–1168., doi:10.1007/s00415-009-5055-0.
- Saleem F, Munakomi S. Pseudobulbar Palsy. [Updated 2020 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553160/
Loading table of contents...
Loading table of contents...
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
New here? Get started!
(Or, click here to learn about our institution/group pricing)1 Month Plan
Full Access Subscription
$142.49
$
94
99
1 Month -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
3 Month Plan
Full Access Subscription
$224.98
$
144
97
3 Months -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
1 Year Plan
Full Access Subscription
$538.47
$
338
98
1 Year -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
Popular
