

An understanding of neuroanatomy is important to success as a neurologist and equally as important for success on the RITE and board exams. In this chapter, you will review key anatomic structures and their functions! We recommend that you review our “Cortex and Connections” chapter prior to reviewing the material outlined below.
Author: Brian Hanrahan MD, James Eaton MD, Steven Gangloff MD
Frontal Lobe Syndromes
Orbitofrontal Syndrome
- Anatomical Function: The orbitofrontal area is involved with voluntary action, decision making, and socially appropriate behavior.
- Exam: Socially inappropriate behavior including Witzelsucht (joking addiction), disinhibition, echopraxia, and utilization behavior (reaching out and using objects in the environment in an automatic manner i.e. reflexively picking up a phone and bringing it to your ear).
Dorsolateral Frontal/Convexity Syndrome
- Anatomical Function: Involved with executive functions, working memory, and selective attention.
- Exam: Poor attention, motor programming, and immediate recall.
Mesial Frontal Cortex Syndrome
- Also called the medial frontal cortex or anterior cingulate circuit syndrome.
- Anatomical Function: The mesial frontal cortex mediates motivated behavior, such as initiation of movement or speech.
- Exam: Amotivation, apathy, and akinesis. Akinetic mutism can be seen in bilateral lesions.
- Patients can be incontinent and may only eat or drink when fed.
- Treatment: Methylphenidate.
Broca’s Aphasia
- Lesion: Posterior inferior frontal gyrus.
- See our language disorders chapter for more information.
Temporal Lobe Syndromes
Kluver-Bucy Syndrome
- Lesion: Bilateral temporal lesions involving the amygdala.
- Exam: Hypermetamorphosis (urge to touch everything), compulsive eating, and hypersexuality.
Prosopagnosia/Visual agnosia
- Failure to identify objects and faces by visual identification.
- Note: may be able to do so by voice.
Wernicke’s Aphasia
- Lesion: Superior temporal gyrus.
- Exam: See our language disorders chapter for more information.
Associations
Broca's = posterior inferior frontal. Wernicke's = Superior Temporal.
Parietal Lobe Syndromes
Dominant parietal lobe
Agraphesthesia (inability to recognize letters or numbers drawn by fingertip on the patient’s skin)
- Astereognosis (inability to recognize an object by touch)
- Ideomotorapraxia (impaired understanding of tool functions i.e. can identify a key but can’t explain what a key does)
Gerstmann’s syndrome
- Lesion: Dominant inferior parietal lobe, AKA dominant angular and supramarginal gyrus of the parietal lobe.
- Exam: agraphia, acalculia, finger agnosia, and left/right confusion.
Non-dominant parietal lobe
- Lesion: Non-dominant angular and supramarginal gyrus.
- Exam:
- Anosognosia (unaware of deficit or illness)
- Sensory or receptive aprosodia (Impaired ability to perceive emotions in others)
- Hemineglect
- Dressing apraxia
Balint’s syndrome
- Lesion: bilateral parietal-occipital lobes
- Exam: (triad)
- Optic ataxia: the inability to move the hand properly to perform voluntary tasks. Visually-guided hand movements are impaired.
- Oculomotor apraxia: the inability to voluntarily fixate eyes to specific locations.
- Simultagnosia: the inability to focus on multiple objects.
- Pathophysiology: Watershed infarcts, multiple embolic strokes, or PRES.
Occipital Lobe Syndromes
Anton Syndrome
- Lesion: Bilateral posterior cerebral artery territory infarction. Can also be seen with PRES.
- Exam: Cortical blindness (the patient has true blindness, but they deny the presence of this blindness).
- Patients will often confabulate in response. For example, if asked to identify the color of something, rather than saying “I can’t see,” they may say “It’s blue.”
Achromatopsia
- Lesion: Inferior lip of the occipital lobe, often bilateral.
- Could also present from a lesion to the thalamus.
- Exam: Colorblindness
Limbic Lobe Syndromes
Apathy
- Lesion: Anterior cingulate.
- Exam: Bilateral lesions can cause akinesis and mutism.
Subcortical Syndromes
Alexia without Agraphia
- Exam: Inability to read, but with retained ability to write.
- Can be seen after a unilateral posterior cerebral artery stroke.
Limb Kinetic Apraxia
- Exam: Inability to perform tasks when asked (i.e. unable to brush hair when given a brush).
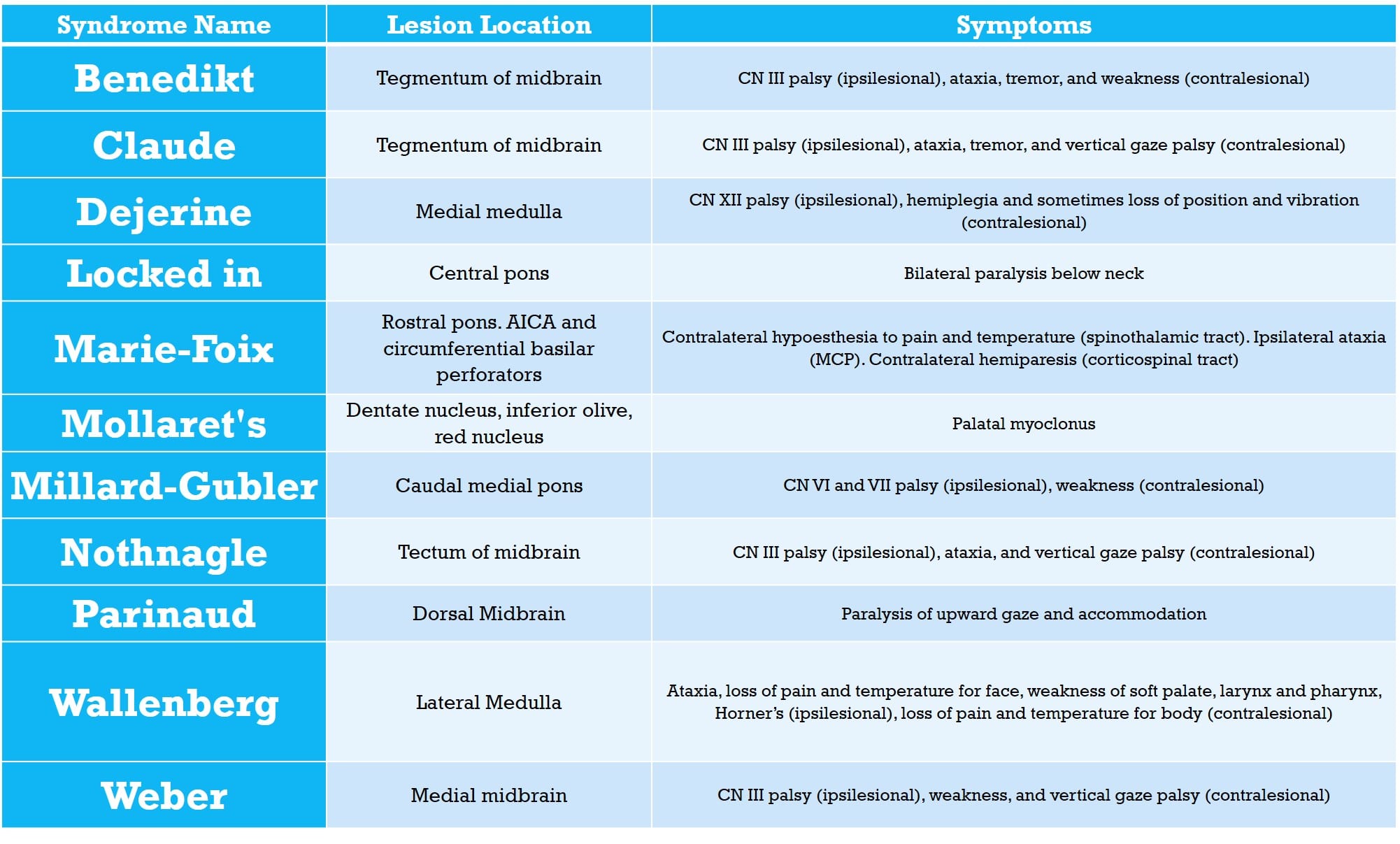
Brainstem Syndromes
Other Syndromes
Charles Bonnet Syndrome
- Seen in patients who have severe vision loss secondary to a variety of pathologies (stroke, macular degeneration, etc.).
- Exam: Complex visual hallucinations without other psychopathology, and with the self-awareness that the hallucinations are not real.
Geschwind Syndrome
(Note: Not to be confused with “Gerstmann Syndrome”)
- A controversial disorder thought to occur in some patients with temporal lobe epilepsy.
- Some researchers question whether it actually exists.
- Presents as a personality syndrome with hypergraphia (compulsive writing), hyper-religiosity, and atypical sexuality (usually hyposexuality).
Alien Hand syndrome
- Presents with uncontrolled movements of an extremity, in the modern era most often seen in corticobasal degeneration, prion disease, and strokes.
- There are three potential areas of localization, which have distinct clinical features as well as most-commonly associated pathologies, as listed below.
- Frontal Variant:
- Dominant hemisphere lesion of the supplementary motor area or medial prefrontal cortex.
- Presents with the right hand impulsively grabbing, groping, and manipulating objects. Also can have utilization behavior.
- Usually follows an ACA stroke.
- Callosal Variant:
- Commonly due to callosal hemorrhage, demyelination, or surgery.
- Often has “intermanual conflict” (antagonizing movements of the two hands).
- Often there are other disconnection symptoms present like apraxia, agraphia, or alexia.
- Posterior variant:
- Secondary to a non-dominant parietal lobe (posterior postcentral gyrus) lesion.
- Associated with a strong feeling of estrangement from the affected limb, and abnormal posturing as well as “levitation” of the limb.
- This variant is the one most commonly caused by corticobasal degeneration, Creutzfeld-Jakob disease, or stroke.
- Frontal Variant:
References
- Campbell WC. Dejong’s The Neurologic Exam. 7th ed. Philadelphia, PA: Lippincott; 2013.
- Crossman AR, Neary D. Cerebral Hemisphere and Cerebral Cortex. In: Neuroanatomy: An Illustrated Colour Text. 5th ed. Philadelphia, PA: Elsevier; 2015:131-145.
- Dronkers, N.F., and Baldo J.V. “Language: Aphasia.” Encyclopedia of Neuroscience, 2009, pp. 343–348., doi:10.1016/b978-008045046-9.01876-3.
- Mega, M.M, and Cummings J.L.“Frontal-Subcortical Circuits and Neuropsychiatric Disorders.” The Journal of Neuropsychiatry and Clinical Neurosciences, vol. 6, no. 4, 1994, pp. 358–370., doi:10.1176/jnp.6.4.358.
- Hausser, Chantal O., et al. “Balint’s Syndrome.” Canadian Journal of Neurological Sciences / Journal Canadien Des Sciences Neurologiques, vol. 7, no. 02, 1980, pp. 157–161., doi:10.1017/s0317167100023544.
- Heimburger, R. F., et al. “Implications of Gerstmann’s Syndrome.” Journal of Neurology, Neurosurgery & Psychiatry, vol. 27, no. 1, Jan. 1964, pp. 52–57., doi:10.1136/jnnp.27.1.52.
- Hurley et al., 2010. “The Brainstem: Anatomy, Assessment, and Clinical Syndromes,” J Neuropsychiatry Clin Neurosci 22(1).
- Kobayashi, Shunsuke, et al. “Clinical Symptoms of Bilateral Anterior Cerebral Artery Territory Infarction.” Journal of Clinical Neuroscience, vol. 18, no. 2, 2011, pp. 218–222., doi:10.1016/j.jocn.2010.05.013.
- Ottomeyer, Caroline, et al. “Aphemia: an Isolated Disorder of Speech Associated with an Ischemic Lesion of the Left Precentral Gyrus.” Journal of Neurology, vol. 256, no. 7, Jan. 2009, pp. 1166–1168., doi:10.1007/s00415-009-5055-0.
- Quint, D. J., and J. L. Gilmore. “Alexia without Agraphia.” Neuroradiology, vol. 34, no. 3, 1992, pp. 210–214., doi:10.1007/bf00596338.
- Trimble, Michael, and Anthony Freeman. “An Investigation of Religiosity and the Gastaut–Geschwind Syndrome in Patients with Temporal Lobe Epilepsy.” Epilepsy & Behavior, vol. 9, no. 3, 2006, pp. 407–414., doi:10.1016/j.yebeh.2006.05.006.
- Sarva H, Deik A, Severt WL. Pathophysiology and treatment of alien hand syndrome. Tremor Other Hyperkinet Mov (N Y). 2014;4:241. Published 2014 Dec 5. doi:10.7916/D8VX0F48
Loading table of contents...
Loading table of contents...
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
New here? Get started!
(Or, click here to learn about our institution/group pricing)1 Month Plan
Full Access Subscription
$142.49
$
94
99
1 Month -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
3 Month Plan
Full Access Subscription
$224.98
$
144
97
3 Months -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
1 Year Plan
Full Access Subscription
$538.47
$
338
98
1 Year -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
Popular
