

Temporal/Giant Cell Arteritis (TA)
- Temporal arteritis (TA) is a granulomatous vasculitis affecting chiefly extracranial arteries of the head (superficial temporal, ophthalmic, etc.) with sparing of the intracranial vasculature.
- Primarily presents in patients over 55 years of age with a headache, scalp tenderness, and jaw claudication. Other symptoms/signs include fever, visual impairment, malaise, myalgia, weight loss, anemia, and tenderness of the temporal artery to palpation.
- Three times more common in women.
- Is often associated with polymyalgia rheumatica.
- Diagnostic workup:
- An erythrocyte sedimentation rate (ESR) should be sent when TA is suspected.
- Will be elevated (>50 mm/hr).
- Temporal artery biopsy
- An erythrocyte sedimentation rate (ESR) should be sent when TA is suspected.
- Imaging may be indicated to exclude other, though less common, compressive causes.
- Treatment:
- Urgent steroid therapy (prednisone) should be started promptly and first to avoid irreversible visual loss, with a temporal artery biopsy to be performed after to provide histologic proof of the diagnosis.
Intracranial Hypotension
- Caused by a CSF leak of the spinal meninges
- Cases can be spontaneous or iatrogenic (lumbar puncture, epidural anesthesia, trauma).
- The most common location for spontaneous CSF leak is the level of the thoracic nerve root sleeves.
- Cases can be spontaneous or iatrogenic (lumbar puncture, epidural anesthesia, trauma).
- Presents with a headache that improves while lying down (aka. “orthostatic headache”).
- Diagnosis:
- CSF opening pressure <6 cm H2O.
- Imaging:
- MRI spine or a CT myelogram (most sensitive)
- MRI brain with contrast may show findings of diffuse dural enhancement and thickening.
- Other possible findings include a downward displacement of the cerebellar tonsils and a decrease in ventriclar size.
- Treatment: blood patch, bed rest, and caffeine. Refractory cases may require neurosurgical intervention.
Cerebral Venous Thrombosis
- Headache is present in up to 90% of cases.
- Can have a migraine or tension-type symptoms, or mimic IIH
- Can have seizures in severe cases.
- Diagnostic workup:
- Vessel Imaging (CTV/MRV)
- MRI/CT head may show parenchymal hemorrhage and/or ischemic stroke.
- Treatment: Anticoagulation +/- surgical thrombectomy in severe cases.

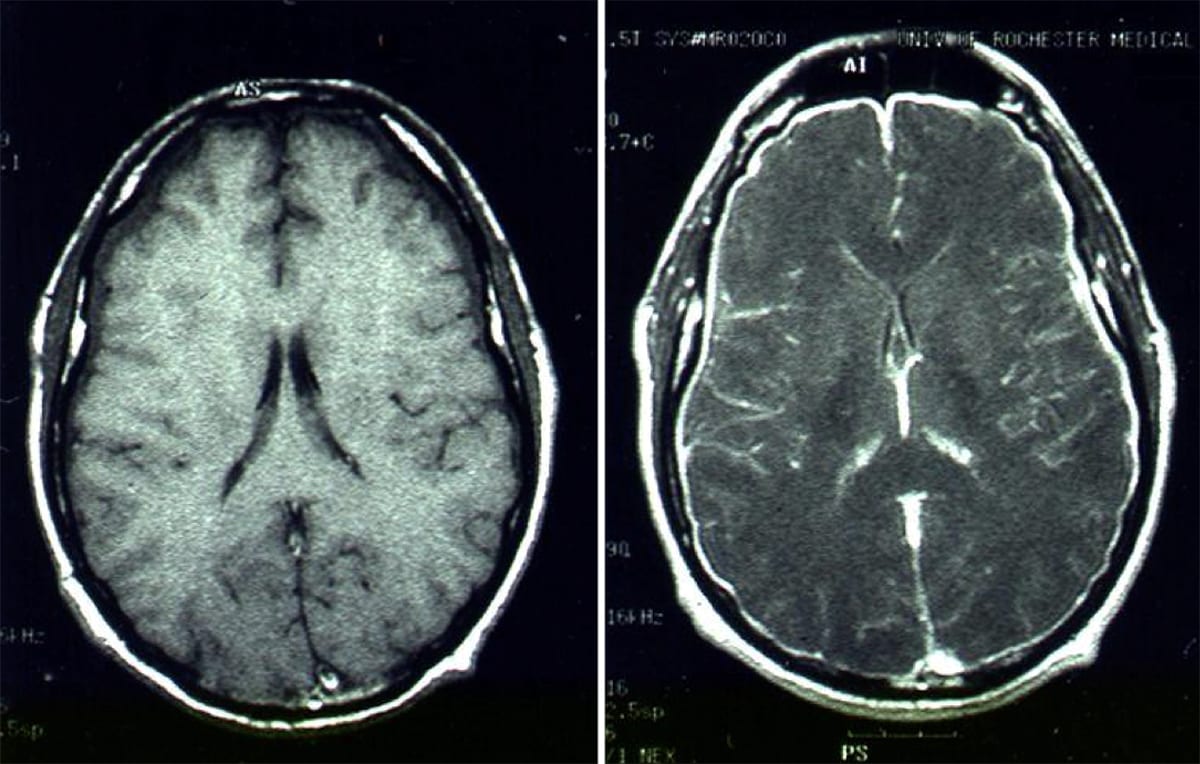
Venous Thrombosis with Hemorrhagic Infarct
Left: Axial T2 FLAIR MRI with hemorrhagic infarct. Right: Sagittal MRV with superior sagittal sinus thrombosis.

Venous Infarct
Caused by a superior sagittal sinus thrombosis.
Subarachnoid Hemorrhage (SAH)
- Classically presents with an acute onset “thunderclap headache” (i.e. intensity increases to its maximum in just seconds) and focal neurology deficits.
- May also be called the “worst headache of life”.
- Other common symptoms include nausea, vomiting, and neck stiffness.
- Diagnosis:
- Lumbar puncture to look for xanthochromia
- CT head
- CTA/MRA
- All SAH patients should have vessel imaging to evaluate for an aneurysm.

Subarachnoid Hemorrhage in the Circle of Willis
Caused by a ruptured berry aneurysm.

Subarachnoid Hemorrhage
Left: Normal axial CT. Right: CT with subarachnoid hemorrhage.

Subarachnoid Hemorrhage with Intraventricular Spread
CT scan, axial cut.

Subarachnoid Hemorrhage with Intraventricular Spread
Axial CT head. Note the blood pooling in the ventricles.

Basilar Aneurysm Rupture
Axial CT with basilar aneurysm rupture. Note the subarachnoid hemorrhage (arrow).

Left MCA Aneurysm Rupture
CT scan, axial cut.

Subarachnoid Hemorrhage from ACA Aneurysm
Left: CT scan, axial cut. Right: Cerebral angiogram.
Medication Overuse Headache (MOH)
- Defined as new or worsening headaches occurring >15 days/month in a patient as a consequence of overusing pain medications for at least 3 months.
- Barbiturates or opiates have the highest association with MOH and thus are never recommended for migraine management.
- Triptans and caffeine-containing compounds can trigger MOH if taken 10 days per month.
- Simple analgesics (acetaminophen, NSAIDs) can trigger MOH if taken 10-15 days per month.
Post-Concussive Syndrome (PCS)
- Seen in patients with mild traumatic brain injury
- Presents with at least three of the following symptoms three week after the inciting injury:
- Headache, fatigue, sleep disturbance, headache, dizziness, irritability, affective disturbance, and apathy.
- Neuroimaging is typically normal
- Most patients with PCS will have symptom resolution within three months.
- Treatment includes reassurance, vestibular-ocular therapy, low-level exercise, and symptomatic treatment of headaches.
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
