

The brachial plexus and innervation of the upper extremities are some of the first topics covered in the first year of medical school. Despite early exposure, physicians regularly rely on reference materials to refresh their memories. Unfortunately, Shelf, RITE*, and Board exams will not let you forget this material. In this chapter, we will discuss the basics of the brachial plexus and upper extremity nerves. Additionally, we will cover commonly seen brachial plexopathies and upper extremity neuropathies.
Authors: Brian Hanrahan MD, Parneet Grewal MD
Brachial Plexus
- The brachial plexus is a network of nerve fibers that relays the motor and sensory information of the upper limbs.
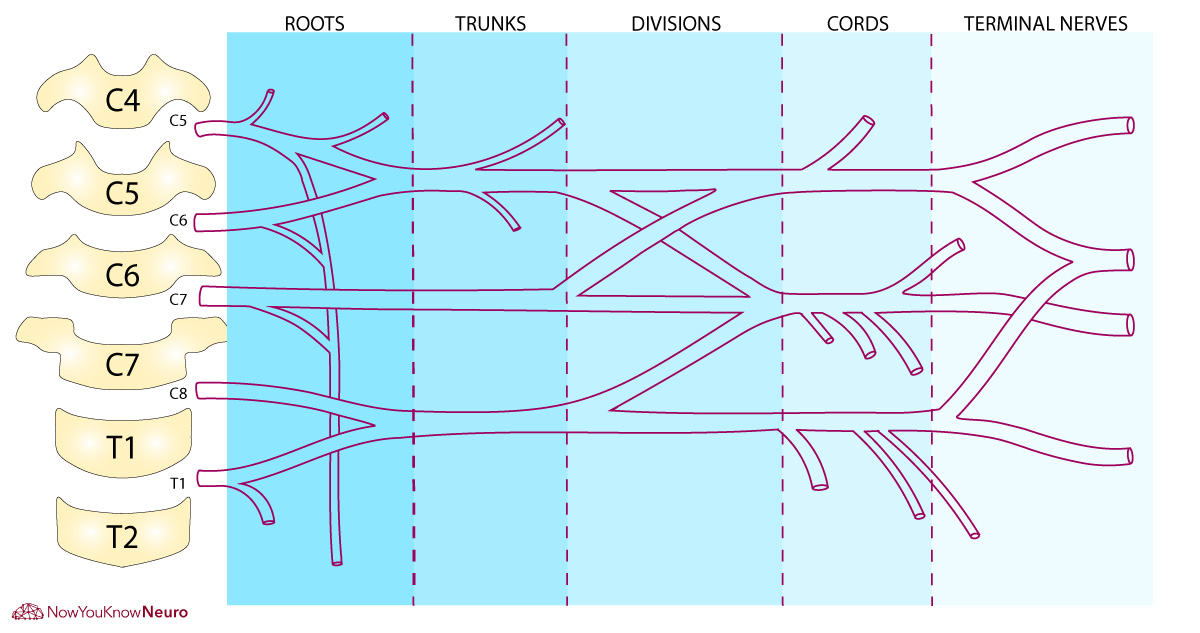
Brachial Plexus Diagram
Move the Slider to Practice!
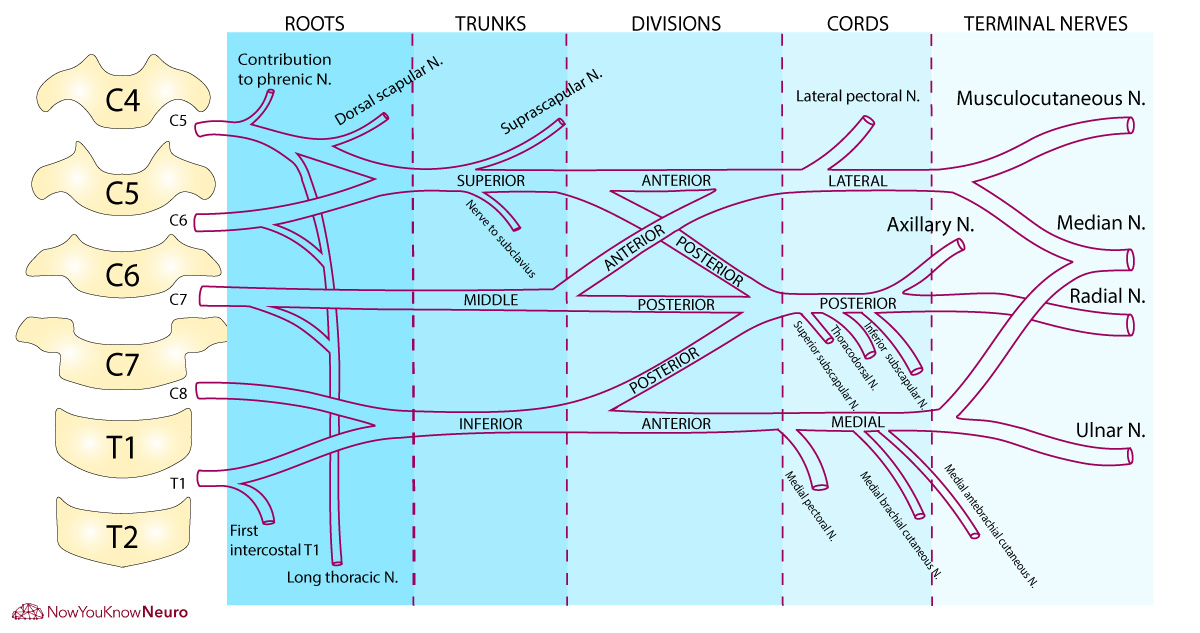
- It is formed by the anterior rami of cervical spinal roots C5, C6, C7, C8, and T1.
- There are 5 sections of the brachial plexus; roots, trunks, divisions, cords, and lastly branches.
- Branches can be considered minor branches or terminal branches (see tables below).
Roots (C5, C6, C7, C8, T1)
- Anterior (motor) and posterior (sensory) roots contribute to the brachial plexus
- Once leaving the intervertebral foramina, roots merge to form three trunks in the neck.
Trunks
- Upper trunk (C5-C6)
- Middle trunk (C7)
- Lower trunk (C8-T1)
- Each trunk splits into anterior and posterior divisions.
Divisions
- Anterior divisions innervate flexor groups.
- Posterior divisions innervate extensor groups.
- Six divisions regroup to become three cords.
Cords
- Lateral cord (C5-C7) is formed from the anterior divisions of the upper and middle trunks.
- Medial cord (C8, T1) is the anterior division of the lower trunk.
- Posterior cord (C5-T1) is formed from the posterior divisions of all three trunks.
- Cords then terminate into terminal branches.
Branches
- Branches of roots
- Dorsal scapular nerve
- Long thoracic nerve
- Branches of trunks
- Suprascapular nerve
- Branches of the lateral cord
- Median nerve
- Musculocutaneous
- Lateral pectoral nerve
- Branches of the medial cord
- Median nerve
- Ulnar nerve
- Medial pectoral nerve
- Medial cutaneous nerve of the arm
- Medial cutaneous nerve of the forearm
- Branches of the posterior cord
- Radial nerve
- Axillary nerve
- Thoracodorsal nerve
- Subscapular nerve
Table 1: Minor branches of the brachial plexus
| Nerve (associated nerve root) | Muscle(s) and function |
| Dorsal Scapular nerve (C5) | Rhomboids: Elevation and adduction of scapula Levator scapulae: Elevation and medial rotation of scapula |
| Subclavian nerve (C5-C6) | Subclavian: Depression of the clavicle and elevation of first rib |
| Long thoracic nerve (C5-C7) | Serratus anterior: Stabilization of scapula against chest wall |
| Suprascapular nerve (C5-C6) | Supraspinatus: Shoulder abduction (first 15 degrees)
Infraspinatus: External rotation of arm |
| Subscapular nerves (C5-C7) | Upper → Subscapularis: Internal rotation of arm Lower → Teres Major: Adduction and internal rotation of arm |
| Thoracodorsal nerve (C6-C8) | Latissimus dorsi: Adduction and internal rotation of arm |
- The rhomboids are solely innervated by the C5 nerve root, This can help differentiate C5 from C6 radiculopathies.
Table 2: Terminal branches of the brachial plexus
| Nerve (associated nerve root) | Muscle(s) and function |
| Axillary nerve (C5-C6) | Deltoid: 15-90 degrees of shoulder abduction
Teres minor: Lateral rotation of arm |
| Musculocutaneous nerve (C5-C7) | Biceps: Elbow flexion and forearm supination
Coracobrachialis: Elbow flexion and adduction of arm Brachialis*: Elbow flexion |
| Median nerve (C5-T1) | Pronator teres: Pronation of forearm
Flexor carpi radialis: Radial flexion of wrist Palmaris longus: Flexion of wrist Flexor digitorum superficialis: Flexion of fingers Flexor pollicis longusª: Flexion of terminal phalanx of thumb Flexor pollicis brevis*: Flexion at proximal phalanx of thumb Flexor digitorum profundus I & IIª: Flexion terminal phalanx of 2,3 fingers Pronator quadratusª: Pronation of forearm Abductor pollicis brevis: Abduction of thumb metacarpal Opponens pollicis: Opposition of thumb metacarpal Lumbricals I & II: Flexion of MCP joints and extension of interphalangeal joints |
| Ulnar nerve (C8-T1) | Flexor carpi ulnaris: Ulnar flexion of wrist
Flexor digitorum profundus: Flexion of hand and fingers Abductor digiti minimi: Abduction of 5th digit Opponens digiti minimi: Opposition of 5th digit Flexor digiti minimi: Flexion of 5th digit Lumbricals III & IV: Flexion of MCP joints and extension of interphalangeal joints Interosseous muscles: Abduction and adduction of fingers Adductor pollicis: Adduction of MCP joint of thumb Flexor pollicis brevis**: Flexion at proximal phalanx of thumb |
| Radial nerve (C5-C8) | Triceps: Extension of forearm
Anconeus: Extension of forearm Brachialis*: Flexion of elbow Brachioradialis: Flexion of elbow Extensor carpi radialis longus: Radial extension of wrist Supinator: Supination of forearm Extensor carpi radialis brevis: Radial extension at the wrist Extensor digitorum: Extensor of MCP joint of 2nd-5th digits Extensor digiti minimi: Extension of MCP joint of 5th digit Extensor carpi ulnaris: Ulnar extension of wrist Abductor pollicis longus: Abduction of MCP of thumb Extensor pollicis longus: Extensor of thumb Extensor pollicis brevis: Extensor of thumb Extensor indicis: Extension of 2nd finger |
MCP: metacarpophalangeal joint, ªInnervated by the anterior interosseous nerve, *Brachialis is innervated by both the musculocutaneous and radial nerves, **Flexor pollicis brevis is innervated by both the median and ulnar nerves.
Brachial Plexus Syndromes
- Presents with pain and/or functional impairment of the ipsilateral upper extremity.
Traumatic plexopathies
- Includes lesions secondary to excessive traction during surgery, gunshot wounds, lacerations, etc.
Erb-Duchenne paralysis/Erb’s palsy
- Occurs secondary to traction or tear of the upper trunk of the brachial plexus (C5 and C6).
- Can be seen with high-energy traction secondary to trauma or iatrogenic traction during difficult child delivery.
- Symptoms include paralysis and atrophy of the deltoid, biceps, and brachialis muscles.
- The arm will hang by the side, medially rotated and with the forearm pronated. This is also known as “Waiter’s tip” palsy.
Klumpke’s palsy
- Occurs secondary to damage of the lower roots (C8, T1) or lower trunk of the brachial plexus.
- Symptoms include paralysis of the intrinsic hand muscles and flexors of the wrist and fingers, producing “claw hand“.
- Other symptoms include numbness of the C8/T1 dermatomes.
- Horner’s syndrome, with ptosis and miosis, can also be seen if the communicating branch to the inferior cervical ganglion is involved (T1).
Thoracic outlet syndrome (TOS)
- TOS arises from compression of the brachial neurovascular bundle which can be vascular, traumatic, or neurogenic in etiology.
- Cervical ribs are the most common cause of thoracic outlet syndrome.
- Compression usually occurs at the lower trunk
- Neurogenic TOS presents with pain, dysesthesias, and weakness in the ipsilateral limb.
- In mild cases, symptoms are only positional, triggered by activity that requires elevation and/or prolonged use of the hands. Severe cases can develop muscle atrophy and significant weakness.
Non-traumatic plexopathies
Idiopathic brachial plexitis (Parsonage-Turner syndrome)
- a.k.a. neuralgic amyotrophy
- Presents with a sudden onset of severe pain in the shoulder which radiates down the arm followed by weakness and sensory loss in the upper extremity.
- Can present in as little as 24 hours but more commonly over two weeks or longer.
- As pain improves, weakness becomes more pronounced.
- The infraspinatus is the most frequently abnormal muscle.
- The long thoracic can often be involved, leading to scapular winging.
- While pain improves usually within 4 weeks, improvement in strength can take several months, even years.
- Triggers can be identified in 50% of cases: Upper respiratory tract infection, vaccination, intravenous drug use, surgery, and childbirth.
- Hereditary brachial plexopathy is an autosomal dominant inherited form of the disorder that presents with relapsing-remitting attacks of brachial plexopathy.
- The prognosis for eventual recovery is good but recovery can take weeks or longer.
- Imaging: MRI of the brachial plexus can show focal thickening, increased T2 signal, and gadolinium enhancement.
- Treatment: Glucocorticoids may be beneficial but overall management is conservative.
Tumor infiltration/neoplastic plexopathy:
- Local tumors (lung and breast cancer) can cause extrinsic compression of the lower plexus.
- MRI can confirm the diagnosis of a mass lesion.
- Lymphoma can infiltrate the brachial plexus but will not show any mass effect on imaging.
Radiation plexopathy
- Seen in patients with a history of malignancy and radiation therapy in the area surrounding the brachial plexus.
Upper Extremity Nerves and Associated Syndromes
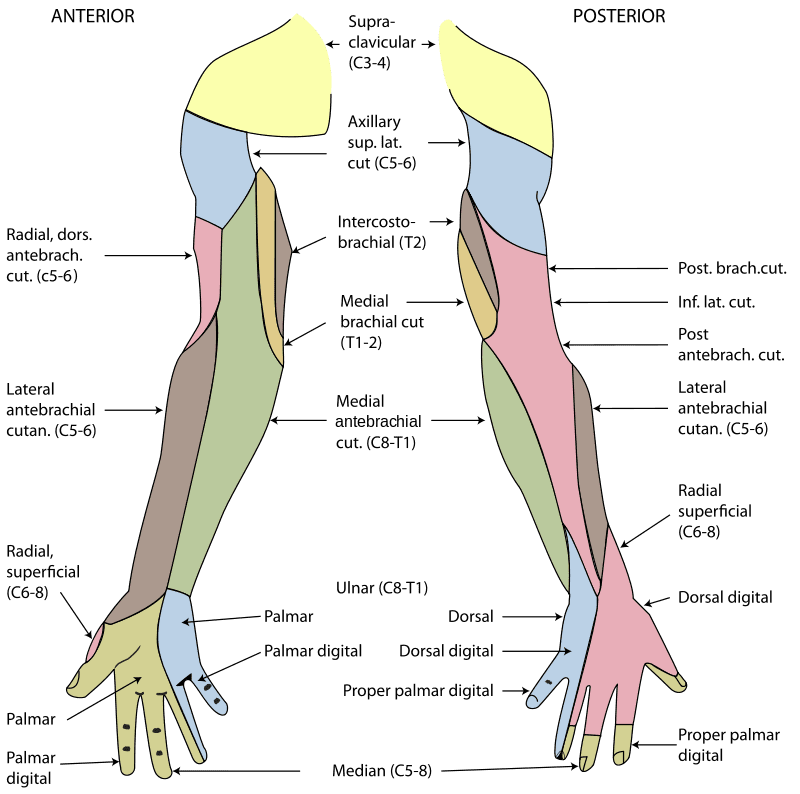
Figure 2: Cutaneous Nerve of the Upper Extremity
Axillary nerve (C5-C6)
- Originates from the posterior cord.
- Travels around the surgical head of the humerus.
- Function
- Motor: Shoulder abduction (15-90 degrees) and external rotation.
- Sensory: Lateral aspect of the upper arm.
- Injury to the axillary nerve can occur with anterior dislocation of the shoulder or humerus fracture at the surgical head.
Musculocutaneous nerve (C5-C7)
- Originates from the lateral cord
- Function
- Motor: Elbow flexion and forearm supination.
- Sensory: Lateral aspect of the forearm via the lateral antebrachial cutaneous nerve.
Radial nerve (C5-C8)
- Originates from the posterior cord.
- Travels through the posterior compartment of the arm along the spiral groove of the humerus and enters the forearm anterior to the lateral epicondyle.
- The triceps and anconeus are innervated above the spiral groove.
- Around the elbow, the nerve bifurcates into a superficial, sensory-only, branch (dorsal digital nerve) and a deep, motor-only, branch (posterior interosseous nerve).
- The posterior interosseous nerve (PIN) supplies the extensor carpi radialis brevis, supinator and all radial nerve innervated intrinsic hand muscles.
- Function:
- Motor: Wrist and elbow extension and forearm supination.
- Additionally, innervation to the brachioradialis is responsible for elbow flexion as well as the brachioradialis reflex.
- Sensory: Lateral dorsum of the hand, dorsal aspects of the first three fingers, and posterior aspect of arm and forearm.
- Motor: Wrist and elbow extension and forearm supination.
Associated syndromes:
Radial neuropathy at the axilla
- Can be seen secondary to compression from using crutches.
- Weakness will be appreciated in all radial associated muscles as well as sensory disturbance of the posterior arm/forearm as well as the dorsum of the hand and first three fingers.
Saturday night palsy
- Most common site type of radial neuropathy.
- Occurs secondary to prolonged compression at the region at the spiral groove or a humerus fracture.
- Presents with wrist drop, finger drop, weakness of flexion (brachioradialis), weakness of supination (supinator), and sensory loss on the dorsal lateral aspect of the hand. Extension at the elbow (triceps) is preserved.
- Generally, the condition will improve spontaneously over a period of weeks to months.
Posterior interosseous neuropathy
- Presents with wrist and finger extension weakness with no sensation loss.
- Triceps, anconeus, brachialis, brachioradialis and extensor carpi radialis longus are spared.
Ulnar nerve (C7-T1)
- Originates from the medial cord.
- Travels from the upper arm into the forearm through the cubital tunnel which is posterior to the medial epicondyle. It terminates in the palm of the hand after passing through Guyon’s canal in the wrist.
- The cubital tunnel and Guyon’s canal are common compression of sites leading to ulnar neuropathy.
- Function
- Motor: Ulnar flexion at the wrist, finger adduction and abduction, adduction of the thumb, and flexion of MCP joints with extension of interphalangeal joints of the 4th and 5th fingers.
- Sensory: Hypothenar eminence and 5th and half of the 4th finger.
Associated syndromes:
Cubital tunnel syndrome
- The most common ulnar nerve injury and the second most common compression neuropathy after carpal tunnel syndrome.
- Presents with pain at the elbow, sensory disturbance of the hypothenar eminence as well as 5th and half of the 4th finger.
- Severe cases develop radial deviation of the wrist upon flexion, due to a weakness of the flexor carpi ulnaris and claw hand deformity, also known as “Pope’s blessing/hand of benediction”, which is due to inability to extend the 4th and 5th fingers normally.
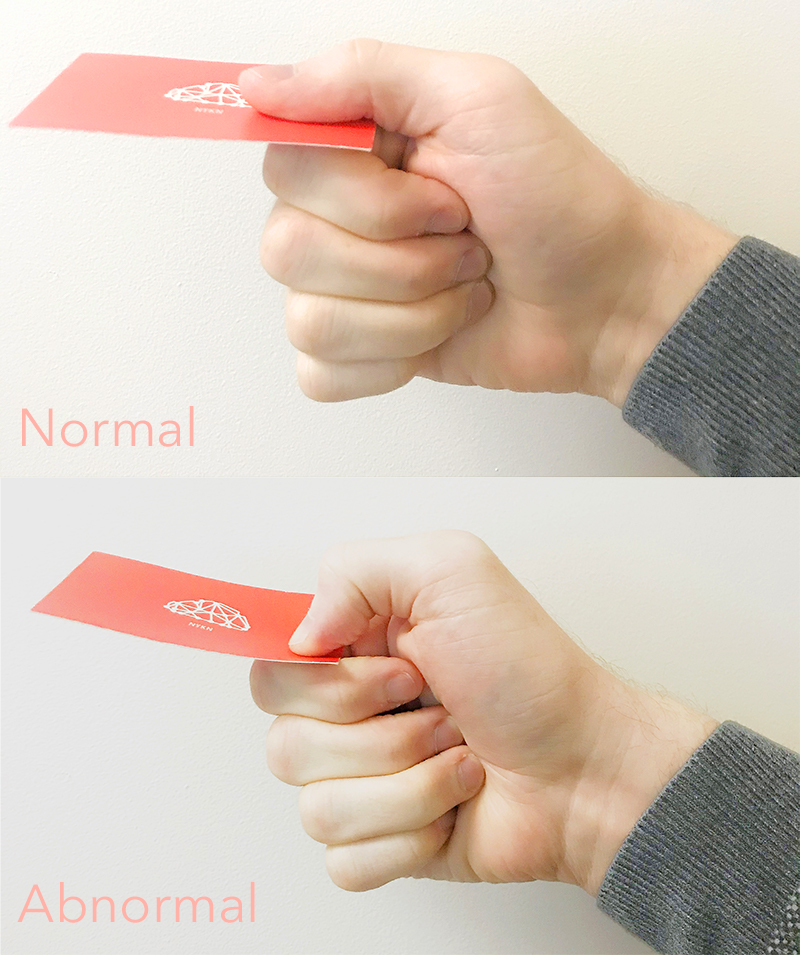
- Froment sign can be present, which tests pinch grip weakness. Pinch grip weakness occurs secondary to adductor pollicis weakness. To compensate, the median nerve innervated muscles, flexor pollicis longus, and flexor digitorum profundus will activate leading to flexion of terminal phalanx’s of the thumb and 2nd finger.
Guyon’s canal syndrome
- Occurs secondary to compression of the ulnar nerve in Guyon’s canal in the wrist.
- Seen in cyclists due to prolonged pressure on the wrist from the handlebars.
- Has comparable symptoms cubital tunnel syndrome, however, forearm strength will be normal.
Median nerve (C5-T1)
- Originates from lateral and medial cords.
- Courses through the anterior arm, forearm, and into the hand via the carpal tunnel.
- The anterior interosseous nerve (AIO) is a pure motor branch of the median nerve that branches off distal to the pronator teres.
- Innervates flexor pollicis longus, flexor digitorum profundus I and II, and pronator quadratus.
- Injury of the anterior interosseous nerve leads to anterior interosseous syndrome (see below).
- The anterior interosseous nerve (AIO) is a pure motor branch of the median nerve that branches off distal to the pronator teres.
- Function
- Motor: Forearm flexion, forearm pronation, finger flexion.
- Sensory: Thenar eminence, proximal palm, palmar aspect of the first 3 digits and half of the 4th digit.
Associated syndromes:
Pronator teres syndrome
- Occurs secondary to compression of the median nerve as it passes through the pronator teres muscle.
- Presents with forearm pain and a sensory disturbance of the lateral palm and 1st-3rd fingers.
Carpal tunnel syndrome (CTS)
- The most common mononeuropathy.
- Occurs secondary to compression to the median nerve as it traverses the wrist through the carpal tunnel.
- Presents with painful paresthesias in the 1st-3rd fingers. Palm sensation is spared due to the branching of the palmar cutaneous sensory branch arising proximal to the carpal tunnel.
- Mild cases only lead to sensory disturbances while moderate and severe cases can lead to weakness and atrophy of the abductor pollicis brevis (APB).
- Other potential weak muscles include opponens pollicis brevis, flexor pollicis brevis, and lumbricals I and II.
- Phalen’s sign or Tinel’s sign may be present.
- More often occurs in the dominant hand and often triggered by sleep or activities that involve prolonged wrist extension or flexion.
Anterior interosseous syndrome
- Presents with forearm pain, forearm pronation weakness (pronator quadratus), terminal phalanx weakness of thumb (flexor pollicis longus), 2nd and 3rd digits (flexor digitorum profundus I and II).
- On exam, patients will be unable to make an “OK” sign due to 1st and 2nd digit weakness.
- Sensation is normal since the anterior interosseous nerve is a pure motor nerve.
References
- Boezaart, Andrép, et al. “Neurogenic Thoracic Outlet Syndrome: A Case Report and Review of the Literature.” International Journal of Shoulder Surgery, vol. 4, no. 2, 2010, p. 27., doi:10.4103/0973-6042.70817.
- “Brachial plexus.” Physiopedia, . 27 Aug 2018, 09:38 UTC. 18 Jan 2019, 22:32 <https://www.physio-pedia.com/index.php?title=Brachial_plexus&oldid=196627>.
- Bromberg MB. Brachial plexus syndromes. Shefner JM, Eichler AE, eds. Uptodate. Waltham, MA: UpToDate Inc. https://www.uptodate.com/contents/brachial-plexus-syndromes (Accessed on January 12, 2019.)
- Louis, Elan D., et al. Merritt’s Neurology. Lippincott Williams & Wilkins, 2016.
- Tharin, Baxter D., et al. “Brachial Plexopathy: A Review of Traumatic and Nontraumatic Causes.” American Journal of Roentgenology, vol. 202, no. 1, 2014, doi:10.2214/ajr.12.9554.
- Weiss, Jay, et al. Easy EMG: A Guide to Performing Nerve Conduction Studies and Electromyography. Butterworth-Heinemann, 2016.
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
New here? Get started!
(Or, click here to learn about our institution/group pricing)1 Month Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
3 Month Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
1 Year Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content

{kind=link}