


Macroscopic anatomy
- The cerebellum contains two lateral hemispheres and a midline vermis.
- It is dorsal to the pons and medulla and separated from the occipital lobe via the tentorium
- Cerebellar hemispheres have marked infoldings forming folia.
- With mass lesions, swelling, or elevated intracranial pressure the cerebellum can herniate through the foramen magnum and compress the brainstem.
- Atrophy of the folia can be seen in patients with chronic alcohol use.

Cerebellar Atrophy
Sagittal section of a cerebellum showing atrophy of the superior part of the vermis secondary to chronic alcoholism.

Cerebellar Atrophy
Low power H&E view of cerebellum showing atrophy of the folia from chronic alcoholism.

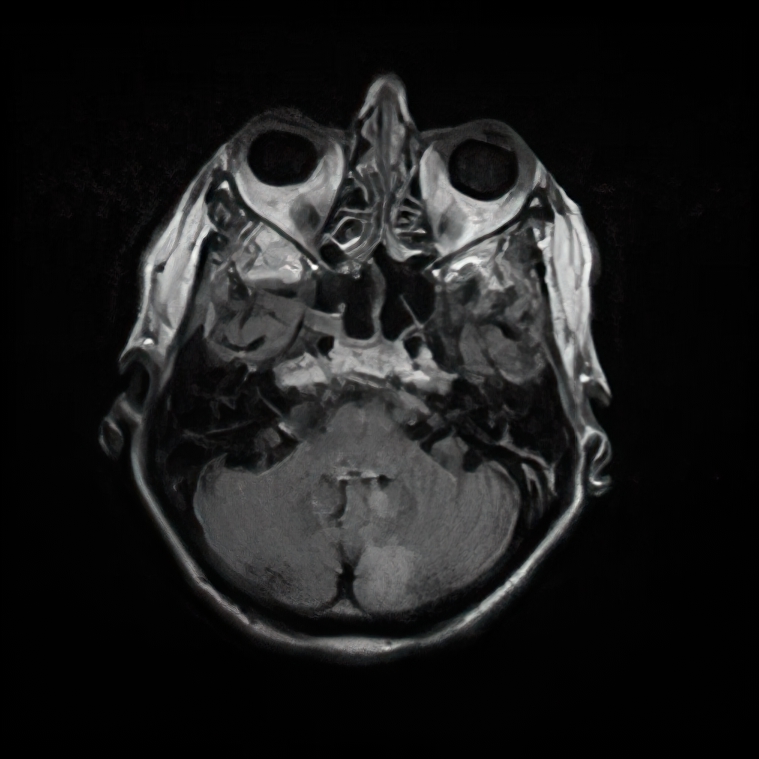
Phenytoin Cerebellar Atrophy
T2 FLAIR MRI axial image.

Cerebellar Tonsillar Herniation
Inferior surface of a gross brain specimen; increased intracranial pressure secondary to brain swelling and/or mass lesion leads to herniation. Herniation of the cerebellum through the foramen magnum shows tonsillar notching (arrows) and eventually necrosis.
Cerebellar Peduncles
- The cerebellum is connected to other brain structures via three paired major white matter tracts: the superior, middle, and inferior cerebellar peduncles.
- The superior cerebellar peduncle contains mostly efferent/output fibers that relay to the thalamus and spinal cord.
- The middle cerebellar peduncle contains input from various regions of the cerebral cortex.
- The inferior cerebellar peduncle primarily contains input from the spinal cord and lower brain stem.
Vascular Supply to the Cerebellum
- Three main arteries provide blood supply to the cerebellum: The posterior inferior cerebellar artery (PICA), anterior inferior cerebellar artery (AICA), and the superior cerebellar artery (SCA).

Cerebellum Vascular Territories
By CFCF – Based upon File:Sobo 1909 655.png, File:Sobo 1909 653.png, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=30644222

Cerebellar vascular supply
This image shows the labyrinthine artery branching off of the basilar, which is actually the second most common variant at <15%. It is more common to branch off of the AICA, which is 85% of cases.
Posterior inferior cerebellar artery (PICA)
- Arises from the vertebral artery.
- This is the largest vascular supply to the cerebellum. It supplies the lateral medulla and most of the posterior and inferior portions of the cerebellum.
- Due to the large vascular supply of the PICA artery, PICA strokes carry a high risk for cerebellar herniation.
- PICA territory strokes are the most common cerebellar stroke. Patients with PICA strokes can present with vomiting, vertigo, horizontal ipsilateral nystagmus, and truncal ataxia. If other PICA-supplied structures are affected patients can present with the lateral medullary syndrome.
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
