


(Note: Gibo and Fisher Classifications number these slightly different)

Anterior Cerebral Artery (ACA)
- The ACA supplies the mesial frontal, medial parietal lobes. There are numerous small perforating branches, including the recurrent artery of Heubner.
- The recurrent artery of Heubner supplies the caudate nucleus and anterior limb of the internal capsule.
- Remember, the posterior limb is supplied by the anterior choroidal artery, a branch directly off of the ICA.
- Both the anterior and posterior limbs also get additional blood supply from the lateral lenticulostriate branches of the MCA.
- The recurrent artery of Heubner supplies the caudate nucleus and anterior limb of the internal capsule.
- The most anterior portion of the ACA is called A1. The A2 segment begins after the anterior communicating artery branches off.
- The anterior communicating artery connects the two anterior cerebral arteries.
- A unilateral ACA occlusion can lead to contralateral weakness and numbness of the lower extremity.
- Other possible symptoms include amotivation, apathy, akinetic mutism, transcortical motor aphasia, alien hand syndrome, and incontinence.

Left ACA Infarct
CT scan, axial view.

Left ACA Infarct
Left: Axial MRI, DWI. Right: DWI, more caudal view.

Remote ACA infarct
Remote infarct weeks to months after the initial injury. There are cystic changes with irregular gray-tan cavities. The bordering parenchyma has slight orange discoloration due to the presence of hemosiderin. These cystic changes can be seen in the ACA vascular territory.
Middle Cerebral Artery (MCA)
- The MCA supplies the temporal lobe, lateral frontal lobe, and most of the parietal lobe.
- Lenticulostriate perforators supply the posterior and anterior limb of the internal capsule, globus pallidus, and corona radiata.
- A posterior limb of the internal capsule stroke can cause contralateral weakness of the face, arm, and leg.
- Lenticulostriate perforators supply the posterior and anterior limb of the internal capsule, globus pallidus, and corona radiata.
- The first segment of the MCA is called M1.
- A proximal M1 lesion can lead to contralateral face/arm weakness/numbness, global aphasia (dominant hemisphere), homonymous hemianopia, and ipsilateral gaze preference.


- An M1 occlusion can sometimes be seen on a CT scan. It is called a “hyperdense MCA sign”.

- CT scan, axial image showing a left hyperdense MCA sign

- The middle cerebral artery (MCA) branches into two major M2 branches, the superior and inferior divisions, in the Sylvian fissure.
- The superior division supplies the lateral inferior frontal lobe, which includes Broca’s area, and the superior parietal lobe.
- Dominant superior M2 infarcts lead to expressive aphasia. Non-dominant superior M2 infarcts can lead to a neglect syndrome such as anosognosia or hemineglect.
- The inferior division supplies the superior temporal gyrus, which includes Wernicke’s area, and the inferior parietal lobe.
- The superior division supplies the lateral inferior frontal lobe, which includes Broca’s area, and the superior parietal lobe.

Right MCA Stroke
CT scan, axial view.

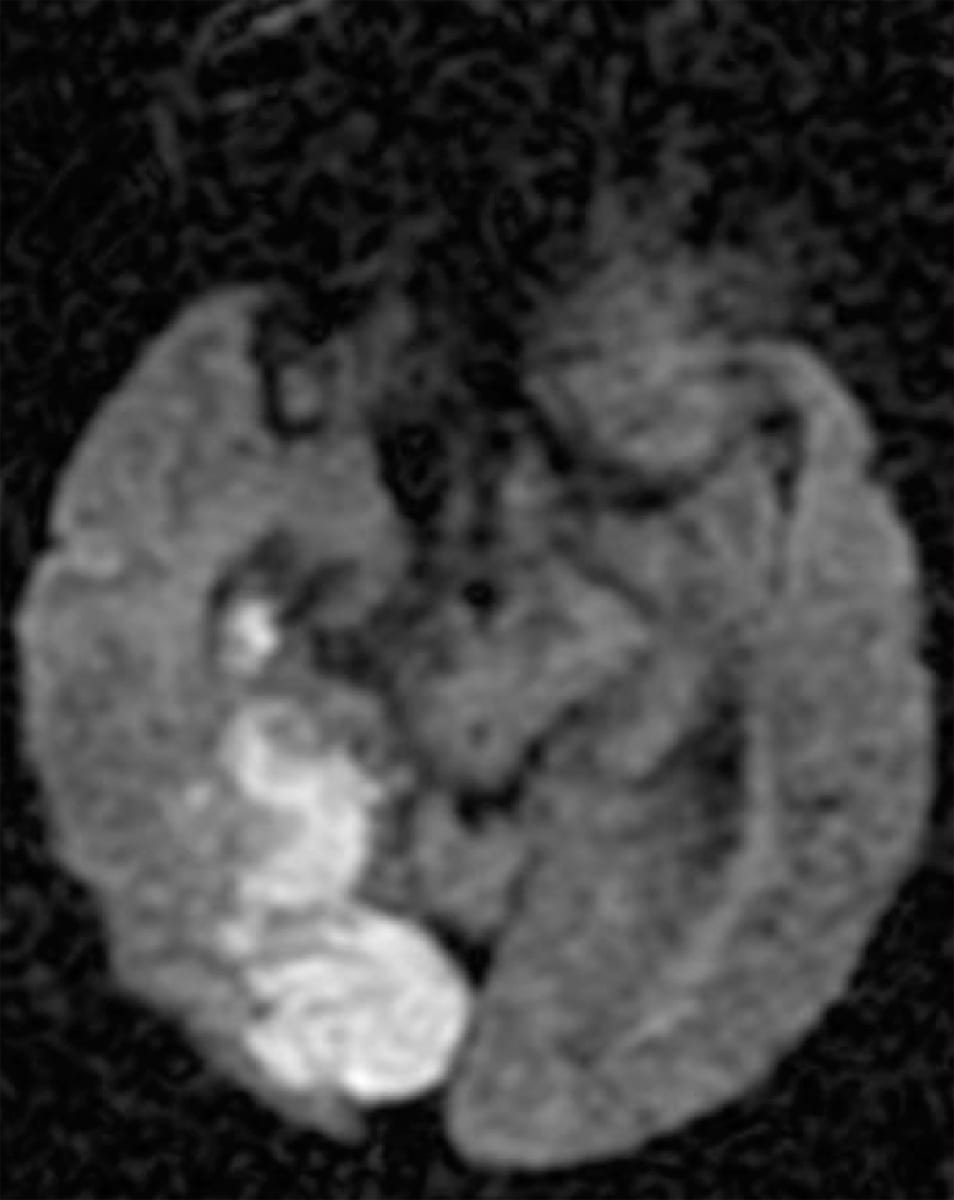
Acute Right MCA Infarct
Axial MRI, DWI sequences.

Acute Left MCA Infarct
Left: Axial MRI, DWI hyperintensity. Right: ADC hypointensity in the same region.

Left MCA Stroke
CT scan, axial view.

Acute Right MCA Infarct
Left: DWI with hyperintensity. Right: ADC with hypointensity.
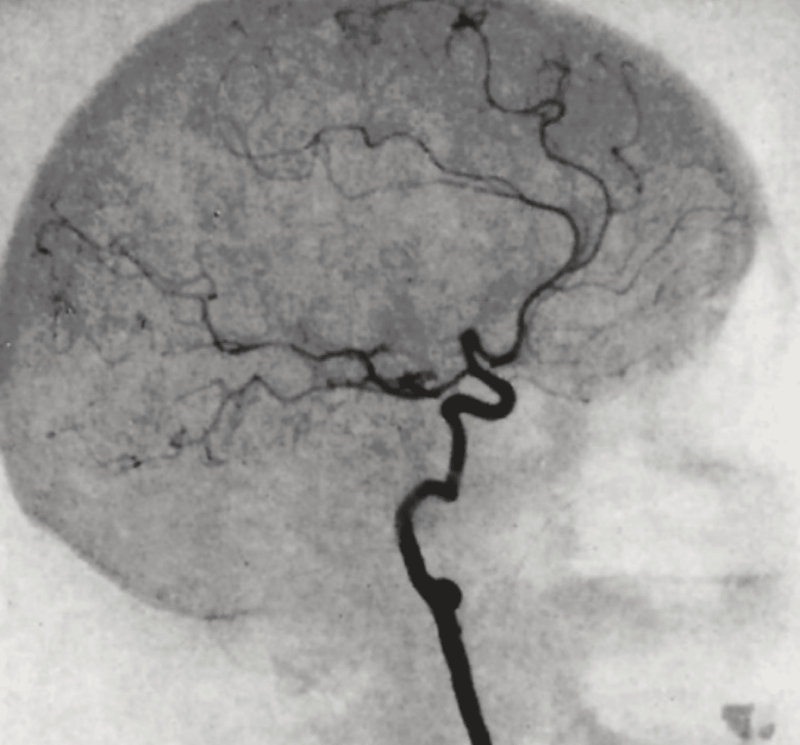
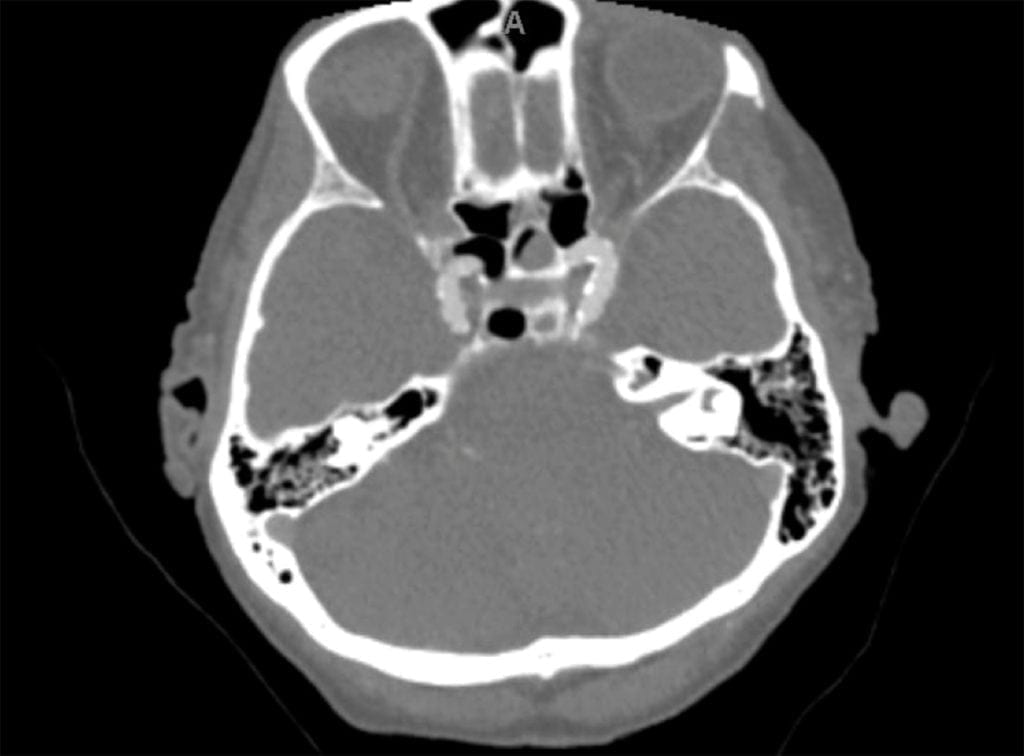
Basilar Artery
- The basilar artery enters the skull along the brainstem and terminates as two posterior cerebral arteries.
- The anterior inferior cerebellar artery (AICA) and superior cerebellar artery (SCA) are key branches of the basilar artery that supply important cerebellar and brainstem regions.
- The AICA supplies the anterior cerebellum, inferior lateral pons, and the middle cerebellar peduncle.
- The SCA supplies the superior cerebellar peduncle, superior portion of the cerebellum, and superior lateral pons
- There are also small pontine perforators off the basilar that supply the medial pons. If injured, these perforators can cause small ischemic strokes that have profound neurological deficits.
- A vessel occlusion at the top of the basilar will lead to coma due to damage to the brainstem as well as possible bilateral medial thalamus damage from blockage of the thalamic-subthalamic arteries (the first branch of the PCA).

- This is a CT angiogram, axial image. Note the two internal carotid arteries anteriorly. Posteriorly, there is no contrast where the basilar artery should be. This is consistent with a basilar artery occlusion.
- Unilateral PCA territory infarcts can present with contralateral homonymous hemianopia, visual agnosia, and/or prosopagnosia.
- Bilateral PCA territory infarcts can present with cortical blindness or Anton syndrome.

Acute Right PCA Stroke
- The circle of Willis represents the arrangement of blood vessels within the brain that allows for collateral circulation. This collateral circulation helps maintain adequate blood flow to brain parenchyma whenever one of its contributing arteries is deficient.
- The ACA, ICA, PCA, anterior communicating, and posterior communicating arteries are considered to be parts of the circle of Willis.
- Branch points between these regions are generally susceptible to the development of saccular aneurysms, especially the anterior and posterior communicating arteries.
- Ruptured aneurysms will cause subarachnoid hemorrhage.

MCA Aneurysm
Cerebral angiogram.

Subarachnoid Hemorrhage from ACA Aneurysm
Left: CT scan, axial cut. Right: Cerebral angiogram.

Left MCA Aneurysm Rupture
CT scan, axial cut.

- Cerebral watershed infarcts, also known as border zone infarcts, involve the regions between two vascular territories.
- They occur secondary to cerebral hypoperfusion or systemic hypotension.
- On imaging, watershed infarcts will present with a “string of pearls” or wedge-shaped regions of ischemia located at the juncture between two vascular territories.
- The two most important ones to know are the ACA-MCA and MCA-PCA territories.
- ACA-MCA watershed infarcts present with ischemia in the frontal lobes
- MCA-PCA watershed infarcts are seen in the parieto-occipital regions.
- Possible clinical presentations for MCA-PCA watershed infarcts include prosopagnosia and Balint syndrome (the triad of simultanagnosia, oculomotor apraxia, and optic ataxia).

ACA-MCA Territory Watershed Infarcts
Axial MRI, T2 FLAIR sequence, showing chronic bilateral watershed infarcts.

Border Zone Infarcts
DWI with hyperintensities between the ACA-MCA and MCA-PCA territories. Note the “string of pearls” pattern of the infarct.

Hypoxic Ischemic Encephalopathy
Axial MRI, DWI sequence.
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
