

Neuro-ophthalmology is a big field in neurology. In fact, it even has its own subspecialty! The pathways involved in vision and eye movements are just as fascinating as they are complex, and for this reason, test makers love to include questions on these topics! Test questions in these fields most often focus on neuro-anatomy and the physical exam and will be covered herein.
Authors: James Eaton, MD, Steven Gangloff, MD, and Brian Hanrahan, MD
The Eye and Retina
- Light passes through the tear film, cornea, anterior chamber, lens, and posterior chamber before reaching the retina.
- Ciliary muscles change the shape of the lens to focus on objects at different distances.
- Once light reaches the retina, it then passes through the nerve fiber layer, ganglion cell layer, inner plexiform layer, bipolar cell layer, outer plexiform layer, photoreceptor (rods and cones) layer, and retinal pigment epithelium.
The Retina
- The retina contains the cone-rich fovea for color vision and a rod-rich region for non-color vision in low light.
- The macula is responsible for central vision and contains many more cones (color vision) than rods (low light vision).
- The fovea has the highest concentration of cones in the macula.
- The outer retina blood supply is by the choroidal circulation, from short ciliary arteries, which are branches of the ophthalmic artery. The inner retina is supplied by the central retinal artery, also a branch from the ophthalmic artery.
- Central Retinal Artery Occlusion (CRAO): Patients will have painless blindness, with a cherry-red spot and narrowed retinal arteries on the fundoscopic exam.
- Causes of CRAO include increased intraocular pressure, embolism, or decreased venous outflow.
- Sudden painless temporary vision loss is called amaurosis fugax.
- The retina is reliant on vitamin A for normal function.
- Vitamin A deficiency is the leading cause of childhood blindness in the world.
- Vitamin A deficiency is the leading cause of childhood blindness in the world.
The Optic disc
- The optic disc is the entry point of the optic nerve into the eye. There are no photoreceptors in the optic disc, and this is the reason for the blind spot in the visual field.
- Increased intracranial pressure can lead to optic disc swelling (papilledema).
- Optic nerve atrophy, as seen after optic neuritis, can cause pallor of the optic disc.

The Pupil and Ocular Autonomic Pathways
- The iris is responsible for controlling the diameter of the pupil, which in turn controls the amount of light that reaches the retina.
- Mydriasis (dilation) and miosis (constriction) of the pupil is dependent on sympathetic and parasympathetic innervation, respectively.
Sympathetic innervation (mydriasis)
- First-order preganglionic neurons from the hypothalamus descend through the lateral brainstem and then synapse in the intermediolateral column of the thoracic spinal cord.
- Second-order preganglionic neurons then project axons to the superior cervical ganglion.
- Axons from the superior cervical ganglia (third-order) neurons travel adjacent to the carotid artery until it diverges within the cavernous sinus. Axons traverse the superior orbital fissure to merge with long ciliary nerves before synapsing on the dilator pupillae muscle.
- Damage along any point of the oculosympathetic pathway (Pancoast tumor, trauma, carotid dissection, etc.) can lead to a Horner’s syndrome (miosis (loss of pupil dilation), ptosis, and anhidrosis).
- Anhidrosis will only occur with 1st order (face and body) or 2nd order (face only) oculosympathetic nerve lesions.

Parasympathetic innervation (miosis)
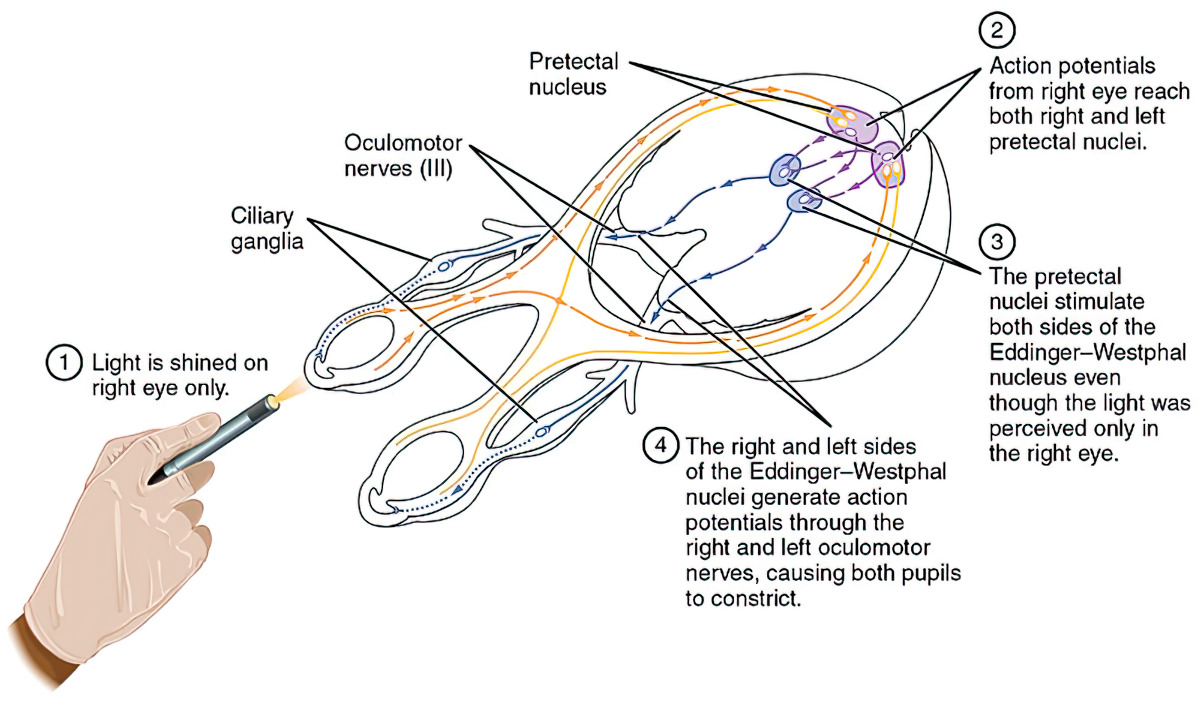
- Optic nerve fibers synapse on the ipsilateral pretectal nucleus, located in the midbrain.
- Pretectal nucleus neurons then synapse on bilateral Edinger-Westphal nuclei.
- The Edinger-Westphal nuclei are responsible for sending preganglionic parasympathetic fibers to the ciliary ganglia.
- Preganglionic fibers from the Edinger-Westphal nuclei travel via the oculomotor nerve and synapse at the ciliary ganglion.
- Due to the superficial location of these preganglionic fibers along the nerve, mydriasis, due to the lack of parasympathetic output to the pupil, is often the first symptom of cranial nerve III compression (uncal herniation, PCOM aneurysm, etc.)
- Cell bodies within the ciliary ganglion then carry postganglionic parasympathetic fibers via the short ciliary nerve to the sphincter pupillae muscle of the iris, to promote miosis.

- Preganglionic sympathetic fibers from the hypothalamus
- Stellate ganglion (no synapse)
- Superior cervical ganglion (sympathetic fibers synapse)
- Carotid plexus with post-ganglionic sympathetic fibers
- Preganglionic parasympathetic fibers (blue) of the oculomotor nerve synapse at the ciliary ganglion
- Postganglionic parasympathetic fibers (dashed green) travel from the ciliary ganglion via the short ciliary nerves to the sphincter pupillae muscle.
- Ophthalmic nerve (yellow) before branching of the long ciliary nerve
- Long ciliary nerve with postganglionic sympathetic fibers (dashed yellow)
- Sphincter pupillae and dilator pupillae muscles of the pupil.
- Pathologic ipsilateral (direct reflex) and/or contralateral (consensual reflex) pupillary constriction can give insight into the integrity of the parasympathetic pathway.
- An optic nerve lesion causes loss to both the direct and consensual reflex.
- Ipsilateral oculomotor nerve or Edinger-Westphal nucleus lesion causes loss of the direct pupillary reflex.
- Contralateral oculomotor nerve and/or Edinger-Westphal nucleus damage causes loss of the consensual pupillary reflex.
The Visual Pathway
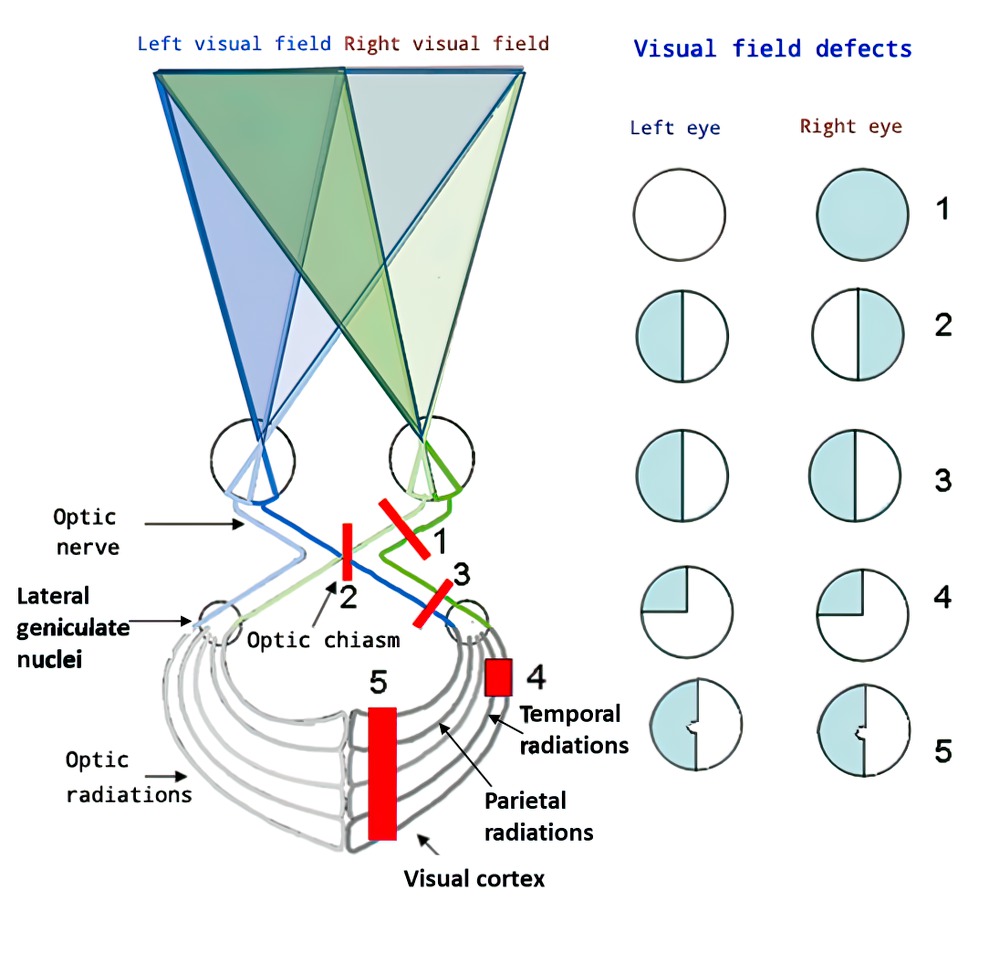
A lot is required of the human body to transform visual stimuli into recognized information. The general pathway taken by a light signal in higher visual processing is retina → optic disc → optic nerve → optic chiasm → optic tracts → occipital lobes.

Visual Pathway Diagram
Move the Slider to Practice!


- The optic nerves travel posteriorly through the back of the globe, enter the orbit, and are invested by meninges. They then come together and decussate at the optic chiasm.
- The optic nerve enters the skull via the optic canal, located superior to the superior orbital fissure shown below.
- The optic chiasm is located in the suprasellar cistern above the diaphragma sellae and the pituitary gland.
- Compression of the optic chiasm from a pituitary adenoma can lead to bitemporal hemianopsia.
- A majority of optic fibers leave the optic chiasm to synapse on the ipsilateral lateral geniculate nucleus (LGN) of the thalamus.
- Some fibers will also synapse on the pretectal nuclei in the midbrain as part of the pupillary light reflex, the superior colliculi to mediate reflexive eye movements, and the suprachiasmatic nucleus to maintain circadian rhythm.
- Third-order neurons leave the LGN as optic radiations through the temporal and parietal lobes.
- Temporal lobe optic radiations are also called Meyer’s loop.
- Optic radiations synapse on the primary visual cortex in the occipital lobe.
- Visual information from the macula synapses on the occipital pole.
- Due to the partially shared blood supply of this region with the middle cerebral artery, posterior cerebral artery territory strokes cause visual deficits that spare central (macular) vision.
Optic Nerve Vascular Pathology
- Anterior ischemic optic neuropathy (AION) presents with monocular visual loss due to hypoperfusion to the optic nerve.
- There are typically two types of AION, arteritic AION (A-AION) and non-arteritic AION (NA-AION).
- Arteritic AION: Occurs due to inflammatory damage to medium-sized blood vessels that supply the optic nerve, and is usually painful.
- An example of arteritic AION is giant cell arteritis, also known as temporal arteritis.
- Non-arteritic AION: Occurs due to non-inflammatory damage to the same blood vessels, and is usually painless.
- The most common causes of NA-AION are small vessel disease risk factors, like diabetes, HTN, and cigarette smoking. NA-AION can also occur after cardiac surgery and is the most common cause of perioperative Ischemic optic neuropathy.
- Arteritic AION: Occurs due to inflammatory damage to medium-sized blood vessels that supply the optic nerve, and is usually painful.
Extraocular Muscles and Cranial Nerves
| Extraocular muscle | Cranial nerve innervation | Function |
| Inferior oblique | Oculomotor (III) | Elevation and extorsion |
| Inferior rectus | Oculomotor (III) | Depression and extorsion |
| Lateral rectus | Abducens (VI) | Abduction |
| Medial rectus | Oculomotor (III) | Adduction |
| Superior rectus | Oculomotor (III) | Elevation and intorsion |
| Superior oblique | Trochlear (IV) | Depression and intorsion |
If you want to learn more about cranial nerves III, IV, and VI check out our Cranial Nerves Chapter!

The Control of Eye Movements
Frontal lobe
- Frontal eye fields, located in the middle frontal gyrus, are responsible for voluntary eye movements.
- Supplied by the superior division of the middle cerebral artery.
- Injury (i.e. ischemic stroke) to the frontal eye field will cause ipsilateral gaze deviation.
- Seizure activity in the frontal eye field will cause contralateral gaze deviation.
Superior colliculus
- Located in the rostral midbrain
- Responsible for coordinating gaze shifts involving eye and head movements.
Paramedian pontine reticular formation (PPRF)
- Located in the pons
- Responsible for coordinating lateral eye movements
- It synapses on the abducens (VI) nerve nucleus which then projects to the ipsilateral lateral rectus via the abducens nerve and also to the contralateral oculomotor (III) nerve nucleus.
- The axons that travel contralateral to the oculomotor nerve nucleus are called the medial longitudinal fasciculus (MLF).
- Axons from the oculomotor nerve nuclei then synapse on the medial rectus, leading to coordinated horizontal eye movements.
Vestibular-ocular reflex (VOR)
- Responsible for coordinating lateral head movements with eye movements to keep objects in focus.
- Changes in head position are relayed from the vestibular nuclei to the abducens nerve. Axons from the abducens (VI) nerve nucleus then project to the ipsilateral lateral rectus via the abducens nerve and also to the contralateral oculomotor (III) nerve nucleus via the MLF.
- Deficits in the VOR may be related to damage to the vestibular nerve, such as in Ménière’s disease, eye movement nuclei (CN VI or CN III), or the MLF.
Vertical Eye Movement
- The rostral interstitial nucleus of MLF (riMLF) is also called the “vertical gaze center” and is located in the rostral midbrain.
- Produces voluntary vertical eye saccades via signals sent first through the frontal eye fields and superior colliculus.
Syndromes with Impaired Eye Movements
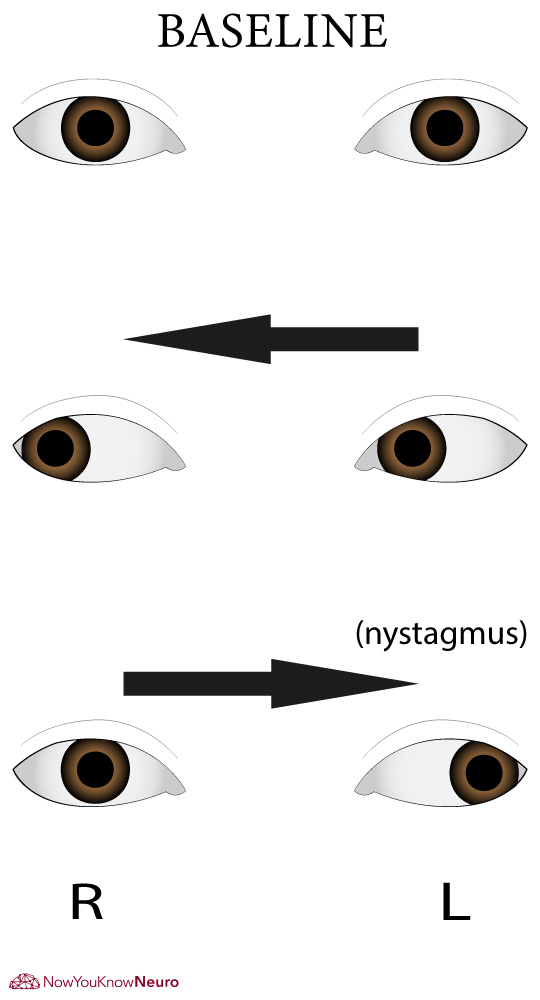
Internuclear ophthalmoplegia (INO)
- A lesion of the MLF leads to ipsilateral adduction weakness and nystagmus in the contralateral eye when looking contralateral to the lesion (i.e. a right MLF lesion will result in adduction weakness of the right eye when the patient looks to the left (see below).
- Causes of INO include infiltrative lesions (tumor, sarcoid, etc.), ischemia, and demyelination.
- Bilateral INO (i.e. Wall-eyed bilateral INO, “WEBINO”) is more commonly secondary to a demyelinating lesion than other pathologies.
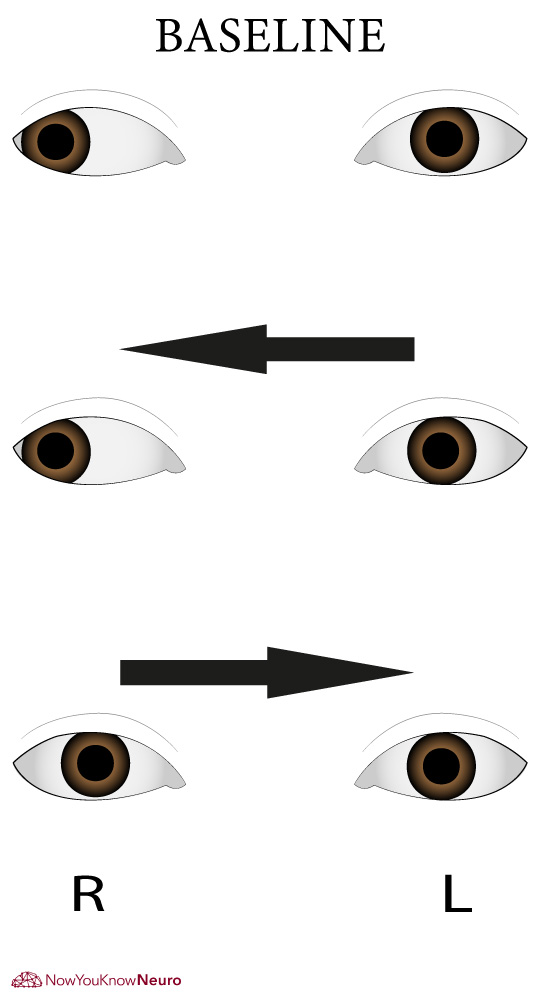
One-and-a-half syndrome
- Seen with injury to the PPRF or the abducens nucleus and the ipsilateral MLF.
- The eye ipsilateral to the lesion(s) will have no lateral eye movements while the eye contralateral to the lesion will only be able to abduct (see below).
Progressive supranuclear palsy (PSP)
- Presents with vertical gaze palsy.
- Brain imaging will show a “hummingbird sign” due to midbrain atrophy.
Parinaud syndrome
- Presents with absent upgaze, light-near dissociation, and convergence paralysis.
- Parinaud’s Syndrome occurs due to compression of the pretectal region of the dorsal brainstem from either a mass lesion or hydrocephalus
Thyroid eye disease
- Also known as Graves’ ophthalmopathy and thyroid-associated orbitopathy, it is an autoimmune disease of the orbit and periorbital tissues.
- Causes extra-ocular muscle enlargement, leading to impaired eye movements.
- Other symptoms include eyelid retraction, lid edema, and proptosis.
Vestibular dysfunction
- Can lead to nystagmus, vertigo, nausea, and imbalance.
- Vestibular lesions will cause nystagmus the fast-beating component moving contralaterally to the lesion (i.e. right-sided vestibular dysfunction leads to left-beating nystagmus).
Other
Diseases with associated eye abnormalities
- Ataxia-telangiectasia:
- Fetal cytomegalovirus (CMV):
- Kearns-Sayre syndrome:
- Myotonic dystrophy:
- Neurofibromatosis type I:
- Neimann-Pick, Tay-Sachs, Metachromatic leukodystrophy, GM1 Gangliosidosis:
- Tuberous sclerosis:
- Von Hippel-Lindau:
- Wilson’s disease:
- Ataxia-telangiectasia: Telangiectasias
- Fetal cytomegalovirus (CMV): Chorioretinitis, keratitis, cataracts
- Kearns-Sayre syndrome: Retinitis pigmentosa
- Myotonic dystrophy: Cataracts
- Neurofibromatosis type I: Lisch nodules, optic nerve glioma
- Neimann-Pick, Tay-Sachs, Metachromatic leukodystrophy, GM1 Gangliosidosis: Cherry red macula
- Tuberous sclerosis: Retinal hamartomas
- Von Hippel-Lindau: Retinal angiomas
- Wilson’s disease: Kayser-Fleischer rings



Drugs with known eye side effects
- Ethambutol:
- Vigabatrin:
- Ezogabine:
- Topiramate:
- Tacrolimus:
- Cocaine:
- Heroin/Opioids:
- LSD:
- PCP:
- Marijuana:
- Methanol:
- Ethambutol: Optic neuropathy
- Vigabatrin: Concentric visual field defects
- Ezogabine: Sclera discoloration
- Topiramate: Acute angle-closure glaucoma
- Tacrolimus: Optic neuropathy
- Cocaine: Mydriasis
- Heroin/Opioids: Miosis
- LSD: Mydriasis
- PCP: Mydriasis
- Marijuana: Conjunctivitis
- Methanol: Vision loss
References
- Berry S, Lin WV, Sadaka A, Lee AG. Nonarteritic anterior ischemic optic neuropathy: cause, effect, and management. Eye Brain. 2017;9:23-28. Published 2017 Sep 27. doi:10.2147/EB.S125311
- Biousse, Valérie, and Nancy J. Newman. “Ischemic optic neuropathies.” New England Journal of Medicine 372.25 (2015): 2428-2436.
- Bouffard MA. The Pupil. Continuum (Minneap Minn) 2019;25:1194-1214.
- Douglas KAA, Douglas VP, Cestari DM. Neuro-ophthalmic manifestations of the phakomatoses. Curr Opin Ophthalmol. 2019;30(6):434-442. doi:10.1097/ICU.0000000000000609
- Hildebrand, Göran Darius, and Alistair R. Fielder. “Anatomy and physiology of the retina.” Pediatric retina. Springer, Berlin, Heidelberg, 2011. 39-65.
- Nautiyal A, Singh S, DiSalle M, O’Sullivan J (2005) Painful Horner Syndrome as a Harbinger of Silent Carotid Dissection. PLoS Med 2(1): e19 doi:10.1371/journal.pmed.0020019
- Prasad S, Galetta SL. Anatomy and physiology of the afferent visual system. Handb Clin Neurol. 2011;102:3-19. doi:10.1016/B978-0-444-52903-9.00007-8
- Phelps PO, Williams K. Thyroid Eye Disease for the Primary Care Practitioner. Disease-a-Month 60(2014)292–298.
- Roth, R A Thisted, J P Erickson, S Black, B D Schreider Eye injuries after nonocular surgery. A study of 60,965 anesthetics from 1988 to 1992. Anesthesiology: 1996, 85(5);1020-7
- Rucker JC. Nystagmus and Saccadic Intrusions. Continuum (Minneap Minn) 2019;25:1376-1400.
- Wray, S., 2014. Eye movement disorders in clinical practice. Oxford: Oxford University Press.
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
New here? Get started!
(Or, click here to learn about our institution/group pricing)1 Month Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
3 Month Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
1 Year Plan
Full Access Subscription-
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
