

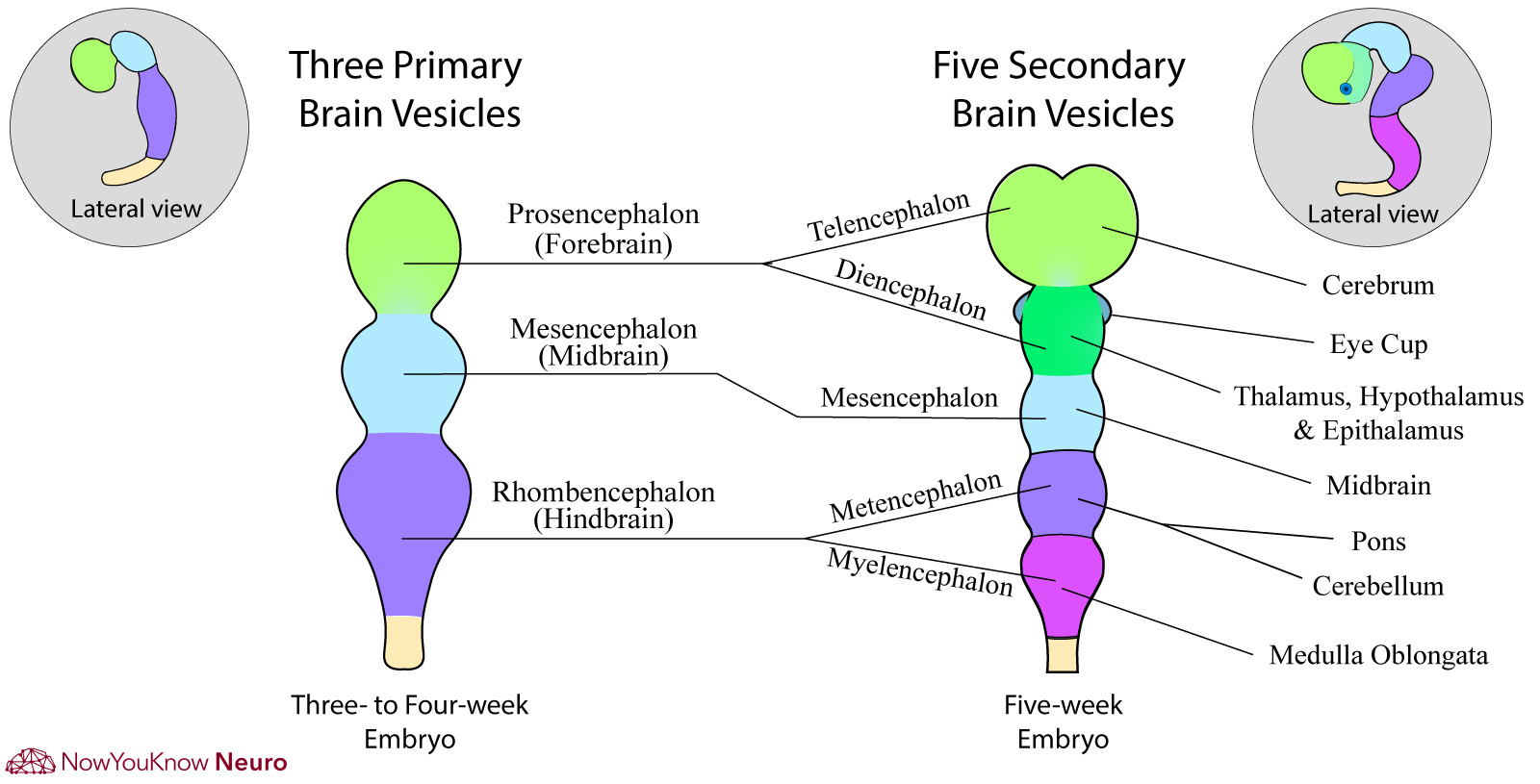
Figure 1: Early Embryonic Development of Nervous System

Neural tube disorders (NTD)
- Neural tube disorders occur during the 4th week of gestation during the closure of the neural tube
- Causes: Genetic factors, folate/B12 deficiency, valproic acid, and carbamazepine exposure.
- Craniorachischisis: Complete failure of neural tube formation leading to both anencephaly and extensive spina bifida.
Anencephaly
- A failure of anterior neural tube closure.
- Usually incompatible with life.
Encephalocele
- Defect of cranial mesoderm development which leads to a skull defect with protrusion of both meninges and brain.
- Associated with Meckel-Gruber syndrome.
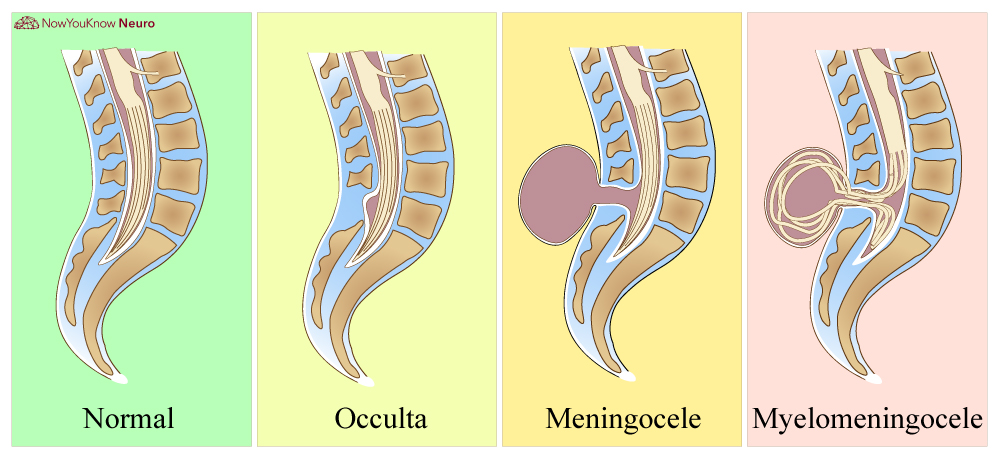
Meningocele
- A pathological opening of the vertebral column in which meninges protrudes through the skeletal defect. No neurologic tissue is herniated outside the spinal cord.
Myelomeningocele (open spina bifida)
- This occurs due to incomplete closure of the caudal neural tube (Figure 3).
- Meninges and spinal cord are both herniated through the defect in a covered membrane. The patient will usually present with significant neurologic impairment.
- If the spinal contents are not covered in a membrane it is called myeloschisis.
Figure 3: Normal spine, meningocele, and myelomeningocele

Myelomeningocele
A large segment of dilated hydromyelic cord is seen within the cystic sac which is covered by skin.

Lumbosacral Myelomeningocele
A flat open lesion consisting of vascular connective tissue and disorganized neural tissue.
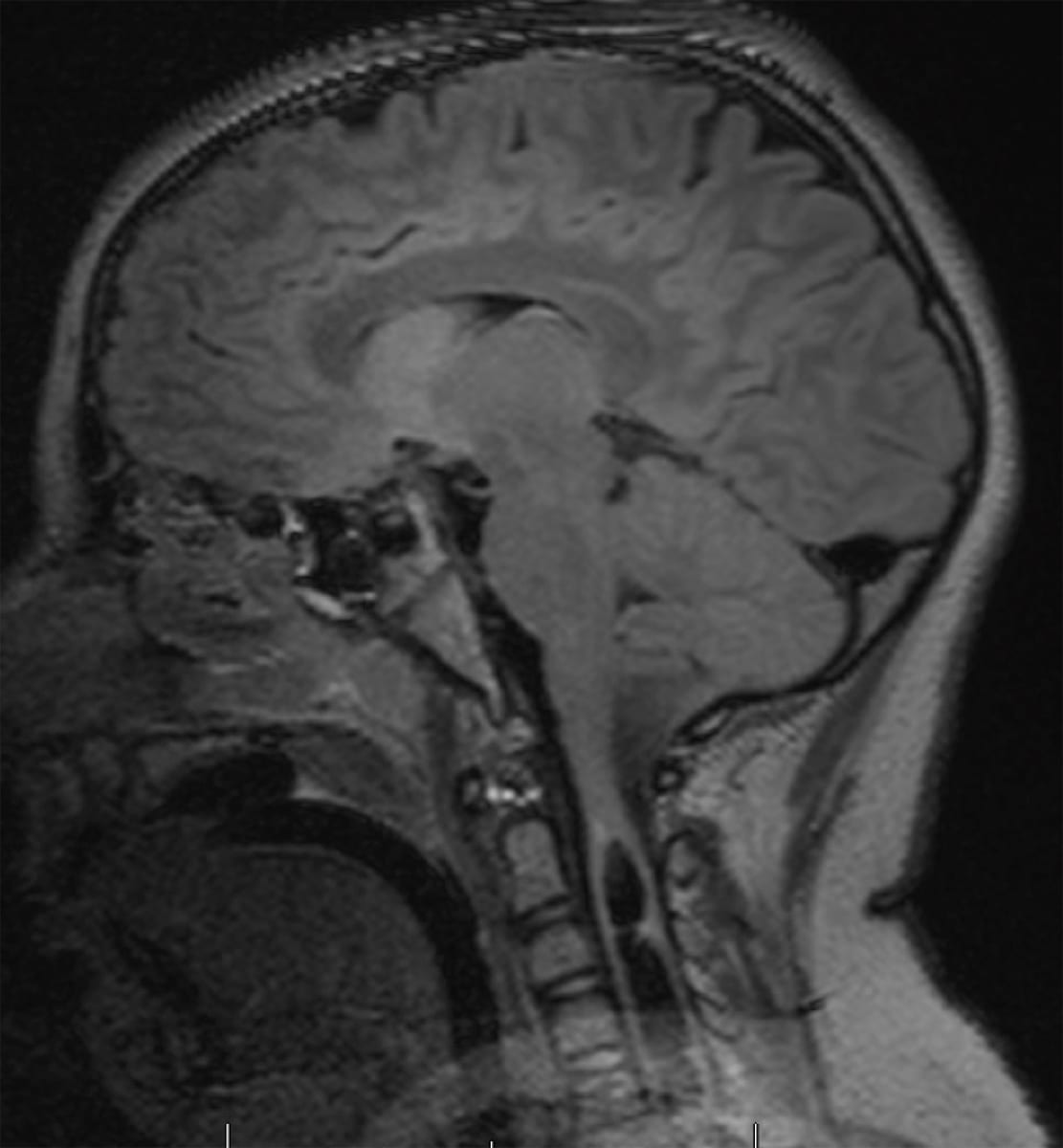
Chiari malformations
- Type I:
- Imaging will show downward displacement of the cerebellar tonsils at least 5 mm beyond the foramen magnum.

Chiari 1 Malformation
Sagittal MRI showing the downward displacement of the cerebellum.

Chiari 1 Malformation
Sagittal MRI showing the downward displacement of the cerebellum.
- Type II:
- Imaging will also show displacement of the cerebellar tonsils as well as the brainstem. Patients can also have a myelomeningocele and are at risk of developing hydrocephalus.
(Type III and IV are not asked often on the shelf, in-service, or board exams)
- Both type I and type II Chiari malformations are associated with syringomyelia, which is an enlargement of the central canal of the spinal cord.
- If symptomatic, patients will complain of loss of pain in a “cape-like” distribution due to damage of the crossing spinothalamic fibers and arm weakness due to damaged anterior horn cells.
Malformations of cortical development
Disorders of cell proliferation/apoptosis:
- Focal cortical dysplasia (FCD) with balloon cells
- FCD can arise from different mechanisms in early development, based on the type and classification system used. For example, FCD with abnormal radial cortical lamination, without balloon cells (FCD Type Ia) occurs typically due to abnormal cortical organization including neuronal migration, while FCD with balloon cells (FCD-type IIb) occurs secondary to abnormal neuronal and glial proliferation during development.
- Megalencephaly
- Microcephaly
Image Gallery of Cell Proliferation/Apoptosis Disorders:

Focal Cortical Dysplasia
Axial T2 FLAIR MRI showing focal hyperintensity of the right parietal cortex.

Focal Cortical Dysplasia
Coronal MRI sequences (T2 left, T1 right) showing an irregular cortical pattern in the left frontal region.
Image Gallery of Cell Migration Disorders:

Lissencephaly
Axial T2 FLAIR MRI showing a near-complete absence of cortical sulci.

Lissencephaly
Axial, T2 FLAIR MRI showing a near-complete absence of cortical sulci.

Nodular Heterotopia
Coronal T1 MRI showing periventricular grey matter.

Nodular Heterotopia
Coronal MRI, T2 sequence, showing periventricular grey matter (heterotopia).

Cortical Heterotopia
Anti-NeuN stained low power view with an abnormal cluster of neuronal grey matter (arrow).
Gallery of Cortical Organization Disorders:

Schizencephaly
Axial MRI showing open-lipped (Type 2) schizencephaly with unfused edges and exposure to the subarachnoid space.

Schizencephaly
Axial MRI T2, showing open-lipped (Type 2) schizencephaly with unfused edges and exposure to the subarachnoid space.
Midline patterning defects
Holoprosencephaly (HPE)
- Caused by the failure of the prosencephalon to develop midline structures.
- Severe cases will have a failure of separation of the cerebral hemispheres.
- Other defects include midline facial anomalies (cyclopia), an absence of the olfactory system, agenesis of the corpus callosum, fused thalamus, and atypical ventricular structure.
- Known to be caused by gestational diabetes, fetal alcohol syndrome, and genetic abnormalities.
- Trisomy 13 is the most common genetic cause of HPE (40% – 60% of HPE of all causes and 75% of HPE due to chromosome abnormality).
- Less common chromosomal causes include trisomy 18 and full triploidy.
Agenesis of the corpus callosum
- Can occur alone or in the context of other developmental abnormalities such as holoprosencephaly.
- Imaging will show a lack of callosal white matter and a dilated third ventricle.
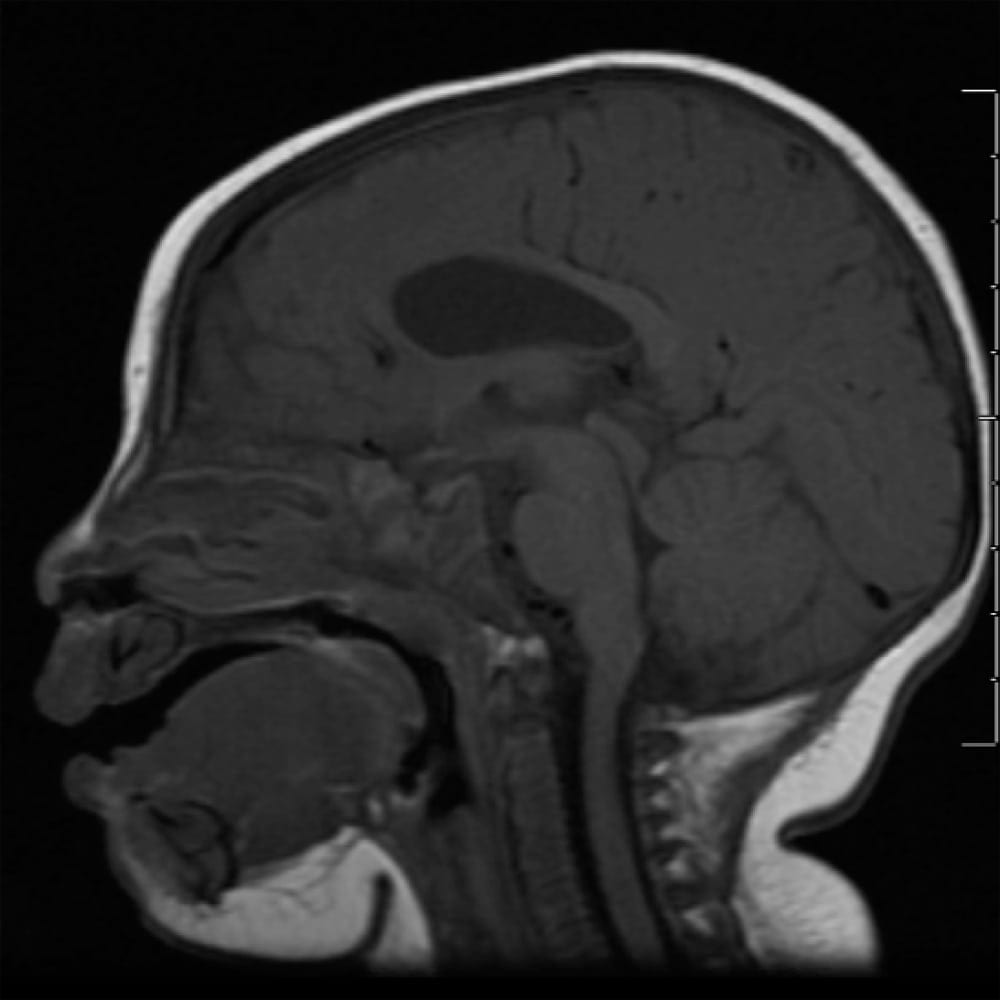
Image Gallery of Midline Pattern Defects:

Holoprosencephaly
Axial FLAIR MRI showing partial fusion of the frontal lobes with an absence of the falx and septum.

Holoprosencephaly
Coronal MRI showing a failure of separation of the cerebral hemispheres.

Alobar Holoprosencephaly
Coronal section.

Septo-optic Dysplasia
Axial MRI, T2 sequence, showing underdevelopment of the optic nerve and absence of the septum pellucidum.

Agenesis of the Corpus Callosum
Sagittal T2-weighted MRI showing agenesis of the corpus callosum.

Septo-optic Dysplasia
Axial T2-weighted MRI; absent septum pellucidum, as seen with septo-optic dysplasia.

Septo-optic Dysplasia
Axial MRI, T2 sequence, showing underdevelopment of the optic nerve and absence of the septum pellucidum.
Cerebellar-specific malformations
Joubert syndrome
- A genetic disorder that presents with cerebellar dysfunction, hyperpnea, and intellectual delay.
- Imaging will show agenesis/underdevelopment of the vermis with the “molar tooth” sign.
Dandy-Walker malformation
- Imaging will show agenesis of the cerebellar vermis, cystic dilation of the fourth ventricle, and elevation of the tentorium.
- Can be associated with other cerebral malformations.

Dandy-Walker Cyst
Left: Sagittal MRI. Right: Axial MRI.

Dandy-Walker Syndrome
CT showing hypoplastic vermis.

Dandy-Walker Malformation
Inferior surface of a gross brain specimen. Note the absent vermis with a widely dilated fourth ventricle with smooth lateral walls and a cystic membranous roof.
Arachnoid cyst
- A space-occupying collection of CSF due to abnormal formation of the leptomeninges.
- If located in the Sylvian fissure, it can appear “box” shaped.
- On imaging, the cyst would be isointense to CSF on all sequences.
- Tend to be clinically silent and only found incidentally.

Arachnoid Cyst
Axial MRI, T1 sequence.

Right frontal arachnoid Cyst
Axial MRI, T2 sequence.

Arachnoid Cyst
Axial MRI.
Porencephalic cyst
- A cavity in brain tissue due to early intrauterine vascular injury or infection.
- The cyst is smooth-walled and not lined by cortex, unlike schizencephaly.
Hydranencephaly
- Imaging will show a large central cyst with a lack of cortical tissue in anterior circulation-supplied areas.
- The cerebellum, midbrain, and basal ganglia tend to be preserved.
- Due to a severe hypoxic/ischemic insult early in development.
- Imaging will show a large central cyst with a lack of cortical tissue in anterior circulation-supplied areas.
Hemimegalencephaly
- Unilateral enlargement of cortex parenchyma with thickened or duplicated grey matter.
- Patients develop epilepsy, intellectual disability, and hemiparesis. If epilepsy is medically refractory, hemispherectomy can be considered.

Hemimegalencephaly
Asymmetric hemispheres with excessive proliferation on the pathologic side.

Hemimegalencephaly
Coronal T1 MRI showing marked parenchymal thickening and asymmetry secondary to excessive neuronal proliferation.
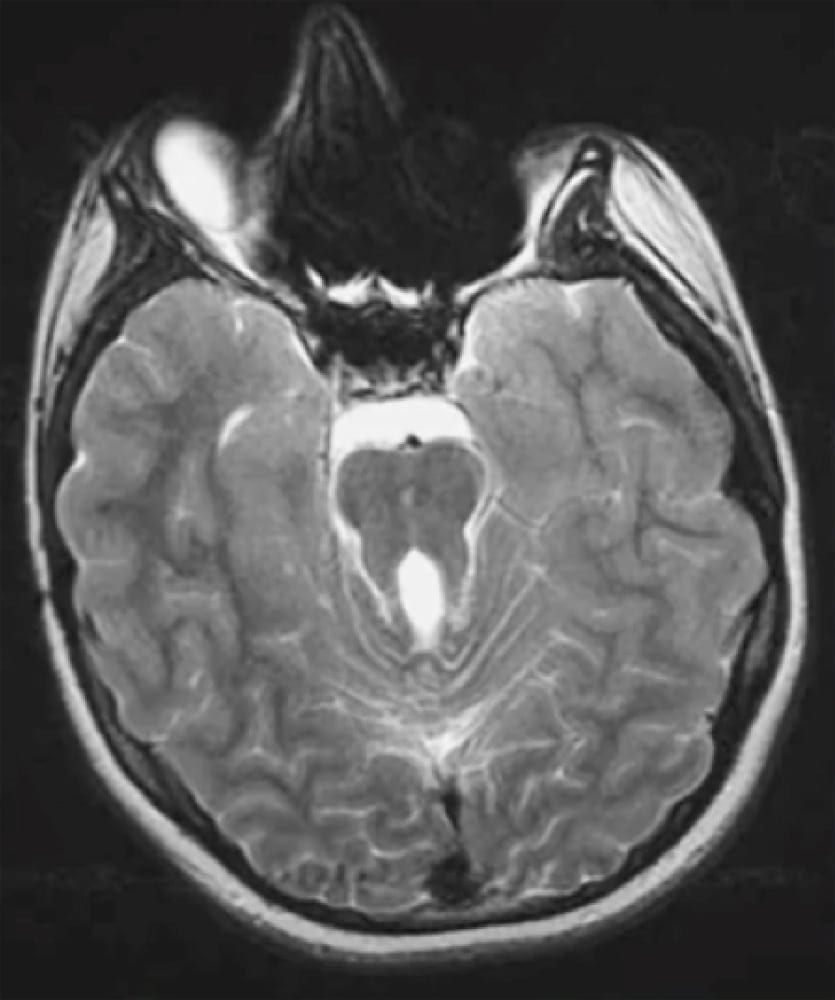
Congenital aqueductal stenosis
- Most commonly due to stenosis of the aqueduct of Sylvius (the narrowest part of the CSF pathway).
- If symptomatic, patients will present with symptoms secondary to hydrocephalus
- Headache, nausea, visual disturbances, altered mental status.
- Enlargement of the circumference of the head if occurs in the first year of life.
- Imaging will show a narrowing of the aqueduct as well as enlargement of the third ventricle and possibly the lateral ventricles.

Congenital Aqueductal Stenosis
Axial CT head showing hydrocephalus likely due to congenital aqueductal stenosis with marked dilatation of both lateral ventricles.

Aqueductal Stenosis
Axial head CT showing severe obstructive hydrocephalus due to aqueductal stenosis.

Ventriculomegaly
Sagittal T2 FLAIR MRI showing severe ventriculomegaly in a 37-week-old patient.
- Treatment: Ventriculo-peritoneal shunt or ventriculostomy.
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
