

Neuromuscular junction diseases, particularly myasthenia gravis, are high-yield for neurology examinations because they command a deep understanding of pathology, diagnostic testing, and therapeutics. Test your knowledge with questions after completing this chapter packed with high-yield facts.
Author: Brian Hanrahan MD
Myasthenia Gravis (MG)
- MG is a postsynaptic autoimmune disease with antibodies directed toward acetylcholine receptors or receptor-associated proteins.
- Patients usually present with weakness, diplopia, dysarthria, and/or dysphagia. Symptoms worsen with sustained or repetitive activity and improve with rest.
- 15% of patients have only ocular deficits referred to as ocular myasthenia gravis.
- Associated with CTLA4 gene single-nucleotide polymorphisms (SNPs) or exposure to ipilimumab.
Diagnostic tests
- Clinical testing
- The ice pack test (placing a bag of ice on a closed lid for two minutes) can be performed to look for improved ptosis as colder temperatures mediate neuromuscular transmission.
- The Tensilon (edrophonium) test can also be done but is rarely performed anymore in clinical practice.
- EMG testing:
- Single fiber electromyography is the most sensitive test for MG (but not specific). If pathologic it will show variable depolarization of a single action potential described as “jitter”.
- Repetitive nerve stimulation at 2 to 3 Hz would show a decrement in compound muscle action potentials (CMAPs) due to the progressive failure of neuromuscular transmission.
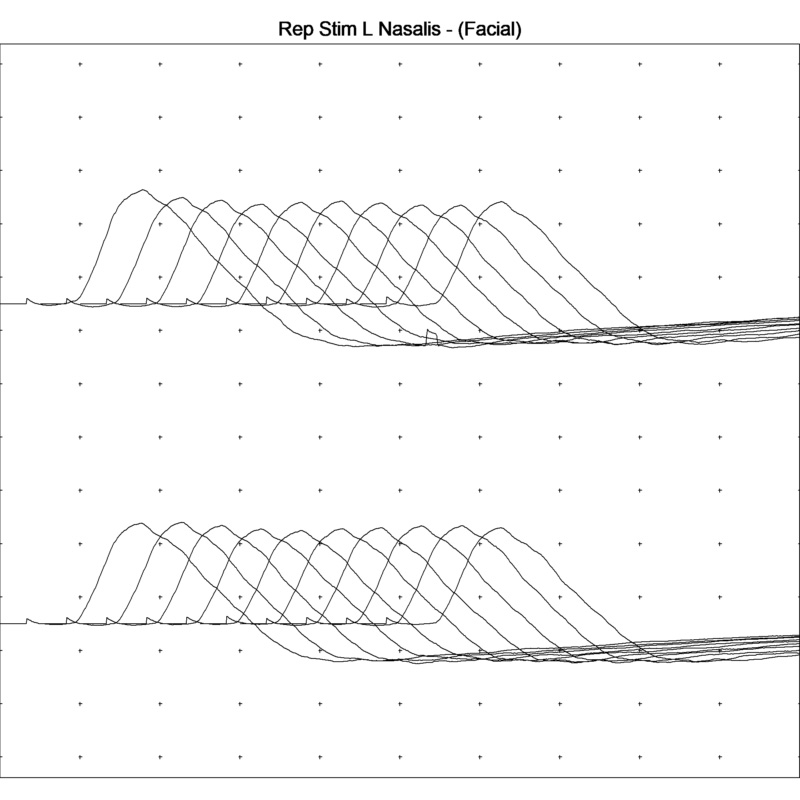
Normal repetitive stimulation testing of the left facial muscles. Action potential amplitudes remain consistent with repeated stimulation.
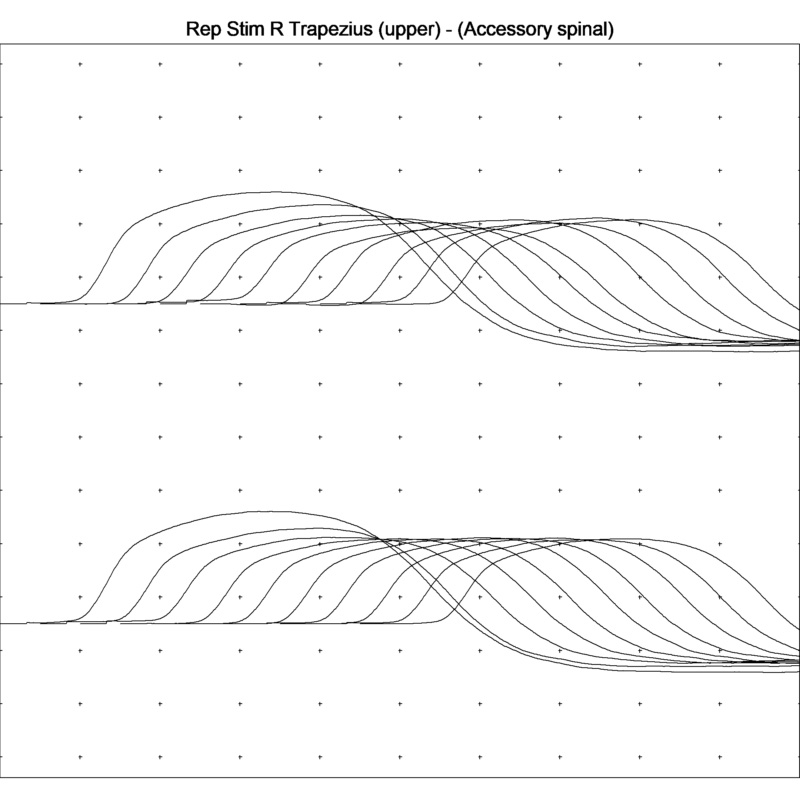
Abnormal repetitive nerve stimulation of the right trapezius muscle. Note the decrement of the action potentials with repeated stimulations.
- Antibody testing:
- ~85% of generalized MG cases and ~50% of ocular MG cases have anti-Acetylcholine receptor (AChR) antibodies
Additional workup
- CXR vs. CT chest to evaluate for thymoma.
Medications to avoid with MG
- Quinolones, tetracyclines, antiarrhythmics, phenytoin, aminoglycosides, beta-blockers, calcium channel blockers, magnesium, lithium, and hydroxychloroquine.
Mnemonic: Please Be Most Concerned About QuALiTy: Phenytoin, Beta Blockers, Magnesium, Calcium channel blockers, Antiarrhythmics, Quinolones, Aminoglycosides, Lithium, Tetracyclines.
Treatment
- The anti-cholinesterase medication pyridostigmine (Mestinon) can produce immediate symptomatic improvement in muscle weakness but has no effect on the immunologic basis of the disorder.
- Can cause cholinergic side effects, including salivation, diarrhea, and vomiting.
- Prednisone is used as first-line therapy for patients with chronic disease but may transiently worsen weakness.
- Intravenous immunoglobulin (IVIG), intravenous methylprednisolone, and plasma exchange (PLEX) are used for acute exacerbations.
- Immunosuppressive agents like azathioprine and cyclosporine have a beneficial effect on weakness, but their benefit takes months to take effect.
- Eculizumab is a complement-binding monoclonal antibody approved for anti-Acetylcholine receptor (AChR) antibody-positive MG
- Requires pretreatment meningococcal vaccine due to an Increased risk of meningococcal infection
- Thymectomy can lead to improvement of MG symptoms regardless if a thymoma is present or not!
Treatment in Pregnancy
- In approximately 40% of women, MG can worsen during pregnancy (typically during the first trimester).
- Acute exacerbation treatment should focus on IVIG. PLEX can be considered as second line. Steroids can be used in the second and third trimester, but may be associated with cleft palate if used in the first trimester.
- Methotrexate (Category X) and mycophenylate (Category D) are contraindicated due to teratogenicity.
- Pre-pregnancy thymectomy should be considered when possible.
Lambert-Eaton Myasthenic Syndrome (LEMS)
- LEMS is a presynaptic autoimmune disease with antibodies directed against voltage-gated calcium channels that impair the acetylcholine release at the neuromuscular junction.
- Patients present with symmetric proximal weakness that improves with repeated use. Reflexes may also improve with exercise.
- LEMS is commonly associated with malignancy, specifically small cell lung cancer (SCLC).
Diagnostic testing
- EMG will show low amplitude compound muscle action potentials (CMAPs) which can increase in amplitude after brief exercise of the tested muscle.
- Like MG, there will be a decline in CMAP amplitudes with 2-Hz repetitive stimulation but there will be an increase in CMAP amplitudes with high frequency (50 Hz) rapid repetitive stimulation.
Treatment
- The potassium channel blocker, 3,4-diaminopyridine (3,4-DAP) (amifampridine) enhances the release of acetylcholine by increasing the duration of the action potential, thus improving motor strength. This is the only currently FDA-approved medication for LEMS.
- If malignancy is found at the time of diagnosis, removal of the tumor can lead to neurological improvement.
- PLEX/IVIG can be used as acute therapy.
What you need to know
Know which diseases are pre-synaptic (LEMS, Botulism, Tick paralysis) vs. post-synaptic (MG)
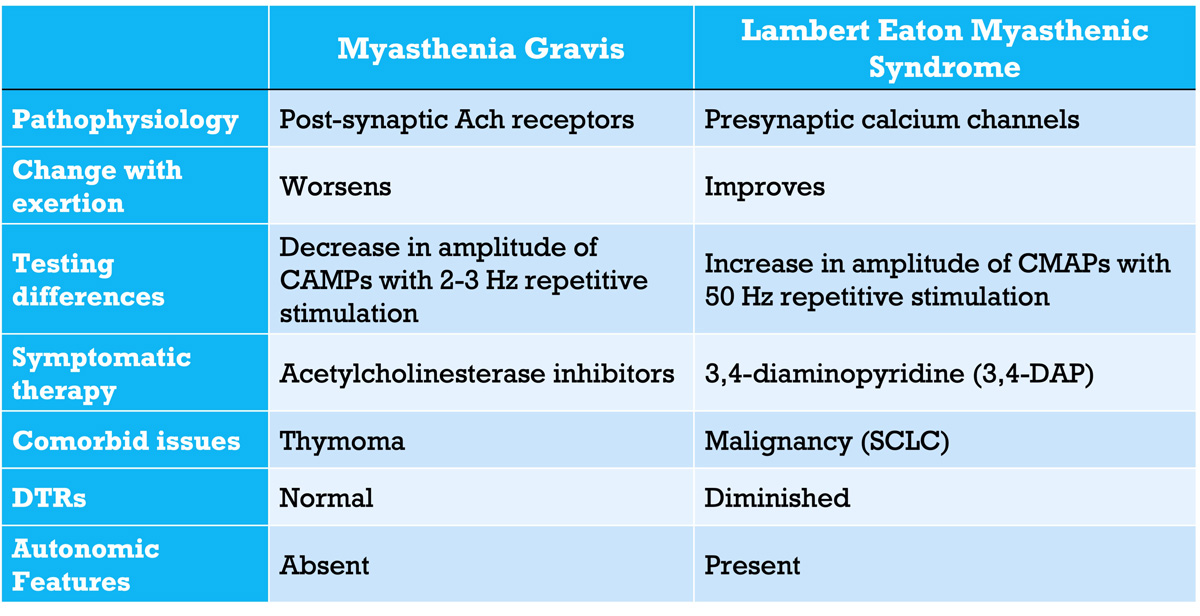
Table 1: MG vs. LEMS
Botulism
- Botulism toxin inhibits the fusion of acetylcholine containing vesicles at the neuromuscular junction in presynaptic neurons by cleaving SNAP/VAMP proteins. These are also sometimes called SNARE (SNAp REceptor) proteins.
- Initially presents with symmetric descending weakness, mydriasis, and decreased tone/reflexes.
- Mydriasis occurs due to botulinum toxin’s effect on both muscarinic and nicotinic cholinergic nerve terminals.
Infantile botulism
- Seen in infants (2-8 months old) due to intestinal colonization of C. botulinum.
- Cases have been linked with exposure to honey or incidental ingestion of C. botulinum spores from the environment (construction site, soil).
- Initial symptoms include constipation, hypotonia, weakness, feeding difficulties, and a weak cry.
Foodborne botulism
- Seen in adults 12 to 36 hours after ingestion of preformed botulinum toxin.
- Exposure to toxins is secondary to home-canned foods and undercooked food.
- Cranial nerve deficits may be the first symptom of descending muscle weakness.
Diagnostic testing
- If EMG is performed, repetitive nerve stimulation (RNS) at 50 Hz will show an incremental response of compound muscle action potentials (CMAPs).
Reminder:
Which diseases are tested via 50Hz repetitive nerve stimulation? ANSWER: Botulism and LEMS
What you need to know:
Confirmatory stool studies are available for infantile botulism, and serum assays for foodborne botulism, however, both studies are not timely and shouldn’t delay treatment.
Tick paralysis
- Caused by a neurotoxin produced in the saliva of Dermacentor tick species in North America.
- The neurotoxin inhibits acetylcholine release at the neuromuscular junction (i.e. presynaptic).
- Patients present with paresthesias and fatigue which then develops into a rapidly progressive painless, ascending weakness with hypotonia and areflexia
- Symptoms are only present while the tick has been on the skin for several days. Removal of the tick results in rapid clinical improvement.
- Diagnostic workup would reveal an embedded tick, normal CSF, as well as normal conduction velocities and SNAPs.
Reminder
Tick paralysis can be confused with GBS due to ascending weakness, however, in tick paralysis, the CSF is normal.
TIP
Suspicion for the disease should be higher during spring and summer months when ticks are more prevalent. Children are more susceptible to this disease than adults.
References
- Bever, Christopher T., et al. “Prognosis of Ocular Myasthenia.” Annals of Neurology, vol. 14, no. 5, 1983, pp. 516–519., doi:10.1002/ana.410140504.
- Jani-Acsadi, Agnes, and Robert P. Lisak. “Myasthenia Gravis.” Current Treatment Options in Neurology, vol. 12, no. 3, 2010, pp. 231–243., doi:10.1007/s11940-010-0070-0.
- Katirji, Bashar. “Clinical Assessment in Neuromuscular Disorders.” Neuromuscular Disorders in Clinical Practice, 2013, pp. 3–20., doi:10.1007/978-1-4614-6567-6_1.
- Odabasi, Z., et al. “Postexercise Facilitation of Reflexes Is Not Common in Lambert-Eaton Myasthenic Syndrome.” Neurology, vol. 59, no. 7, Aug. 2002, pp. 1085–1087., doi:10.1212/wnl.59.7.1085.
- Pegram P, Stone S. Botulism. UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on 10/10/2018.) www.uptodate.com/contents/botulism.
- Pestronk, Alan. Neuromuscular Home Page, neuromuscular.wustl.edu/index.html.
- “Randomized Trial of Thymectomy in Myasthenia Gravis.” New England Journal of Medicine, vol. 375, no. 20, 2016, pp. 2005–2007., doi:10.1056/nejmc1611704.
- Sanders, D. B., et al. “Clinical Aspects of MuSK Antibody Positive Seronegative MG.” Neurology, vol. 60, no. 12, 2003, pp. 1978–1980., doi:10.1212/01.wnl.0000065882.63904.53.
- Sanders, D. B., et al. “Single-Fiber Electromyography in Myasthenia Gravis.” Neurology, vol. 29, no. 1, Jan. 1979, pp. 68–68., doi:10.1212/wnl.29.1.68.
- Singer, S., et al. “Posterior Reversible Encephalopathy Syndrome in Patients With Cancer.” The Oncologist, vol. 20, no. 7, Jan. 2015, pp. 806–811., doi:10.1634/theoncologist.2014-0149.
- Weimer T, Gutmann L. Overview of neuromuscular junction toxins. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on 10/10/2018.) https://www.uptodate.com/contents/overview-of-neuromuscular-junction-toxins
- Wendell, Linda C., and Joshua M. Levine. “Myasthenic Crisis.” The Neurohospitalist, vol. 1, no. 1, 2011, pp. 16–22., doi:10.1177/1941875210382918.
- Pevzner, A., Schoser, B., Peters, K., Cosma, N. C., Karakatsani, A., Schalke, B., … & Kröger, S. (2012). Anti-LRP4 autoantibodies in AChR-and MuSK-antibody-negative myasthenia gravis. Journal of neurology, 259(3), 427-435.
- Suzuki, S., Utsugisawa, K., Nagane, Y., & Suzuki, N. (2011). Three types of striational antibodies in myasthenia gravis. Autoimmune diseases, 2011.
- Sanders, D. B., Wolfe, G. I., Benatar, M., Evoli, A., Gilhus, N. E., Illa, I., … & Nicolle, M. (2016). International consensus guidance for management of myasthenia gravis: executive summary. Neurology, 87(4), 419-425.
- Chaudhry, Shahnaz Akhtar et al. “Myasthenia gravis during pregnancy.” Canadian family physician Medecin de famille canadien vol. 58,12 (2012): 1346-9.
- Varner, M., Myasthenia Gravis and Pregnancy, Clinical Obstetrics and Gynecology: June 2013 – Volume 56 – Issue 2 – p 372-381
doi: 10.1097/GRF.0b013e31828e92c0 - Batocchi AP, Majolini L, Evoli A, et al.. Course and treatment of myasthenia gravis during pregnancy. Neurology. 1999;52:447–452.
- Gilhus, Nils Erik, et al. “Myasthenia Gravis.” Nature Reviews Disease Primers, vol. 5, no. 30, 2019, pp. 1-19.
Loading table of contents...
Loading table of contents...
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
New here? Get started!
(Or, click here to learn about our institution/group pricing)1 Month Plan
Full Access Subscription
$142.49
$
94
99
1 Month -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
3 Month Plan
Full Access Subscription
$224.98
$
144
97
3 Months -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
1 Year Plan
Full Access Subscription
$538.47
$
338
98
1 Year -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
Popular
