

Glasgow Coma Scale (GCS)
- GCS ranges from 3 (profoundly comatose) to 15 (normal).

- Common causes of TBI include falls, motor vehicle accidents, assaults, explosive blasts, and penetrating injuries.
- The more severe the TBI, the higher the risk for the development of focal epilepsy.
- Radiographic findings consistent with TBI:
- Skull fractures
- Cerebral contusions, typically in areas where brain parenchyma rubs against skull bone (i.e. inferior temporal and frontal lobes)
- Coup contusions occur on the side of the trauma.
- Countercoup contusions occur on the opposite side of the site of impact.
- Pneumocephalus due to penetrating injury or skull fracture.
- Can be associated with pneumolabrinth (air in the inner ear).
- Cerebra edema

Acute Brain Contusion

Contrecoup Contusion

Old Inferior Frontal Lobe Contusions

Cerebral Contusion
Axial CT head.
Diffuse axonal injury
- Due to shearing forces from extreme acceleration and deceleration.
- A biopsy will have swollen proximal ends of axons in the appearance of bulbs known as “retraction balls.” Punctate hemorrhages may also be seen.
Basilar skull fracture
- Battle’s sign (ecchymosis of the mastoid region) and raccoon eyes (periorbital ecchymosis) may be seen.
- May also have leakage of CSF from the ears (otorrhea) or nose (rhinorrhea).
- Can test rhinorrhea or otorrhea for β-transferrin, to determine if a CSF leak is present, as this is only positive in CSF.
Non-accidental trauma in a child
- Suspicious signs include spiral fracture of the humerus, immersion burns, rib fractures, retinal hemorrhages (from shaking), long bone injuries, duodenal hematomas, brain contusions, subdural hematoma, and skull fracture.
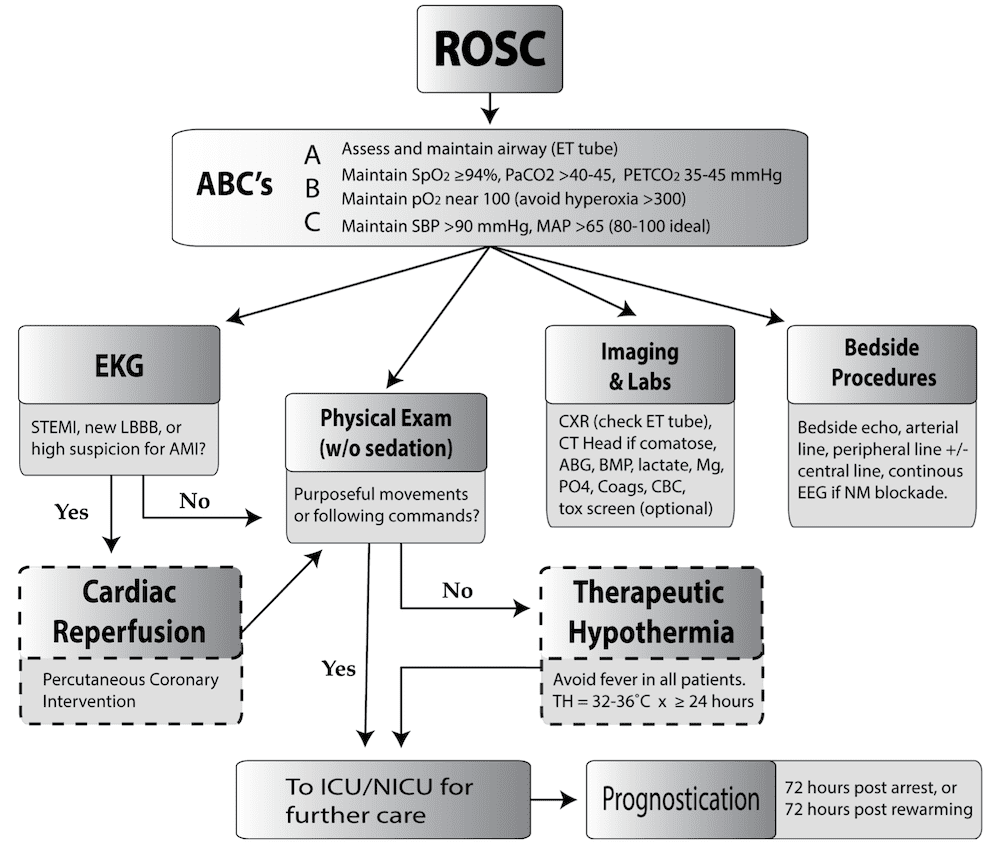
Goals
- Optimize organ perfusion
- Optimize ventilation
- Optimize temperature.
- Identify the cause of arrest
- Prognosticate
Ventilation
- Low PaCO2 can cause cerebral vasoconstriction, so avoid hyperventilation.
- Hyperventilation lowers PaCO2
Circulation
- Optimize cerebral perfusion using a target MAP (mean arterial pressure)
- Norepinephrine or other catecholamines can be used. Dobutamine or milrinone can be used to increase cardiac output if global hypokinesia of the heart is seen on echocardiogram.
Physical exam
- Tachycardia is expected after return of spontaneous circulation (ROSC) is achieved.
- If bradycardia is seen, consider hypoxia or metabolic disturbance.
Treatment
- Therapeutic hypothermia
- Cool to 32-36° C for ≥24 hours
- Propofol and fentanyl decrease shivering, which can help to decrease body temperature.
- After cooling, re-warm
- Monitor for cardiac arrhythmias (bradycardia, atrial fibrillation, ventricular tachycardia).
- Most common complication during hypothermia protocol
- Glucose control
- Keep between 140-180 mg/dL.
- PCI
Prognostication
- Prognostication should be performed at 72 hours post-arrest or 72 hours post-re-warming
- Continuous EEG may aid in prognostication.
- Risk factors for poor prognosis after cardiac arrest:
- Bilateral absence of N20 response on somatosensory-evoked potentials is the strongest predictor of a poor outcome.
- Longer time to ROSC
- Absence of brainstem reflexes 3 days post-resuscitation
- Extensor or no motor response
- Lower pH and/or higher lactate
- Elevated neuron-specific enolase
- Hypotension requiring >2 vasopressors
- Absence of reactivity on EEG
- Burst-suppression pattern on EEG
- Burst-suppression or a low voltage (<20 µV) EEG at 24 hours post-arrest has been reported to have a 99-100% chance of a poor outcome.
- Normal background without discharges has been reported as high as a >70 % chance for a good outcome.
Intracranial Pressure (ICP)
- Normal ICP is 5-15 mmHg.
- Increases in pCO2 cause vasodilation and thus increase ICP.
- Hyperventilation causes decreased pCO2 and therefore decreased ICP. This can be helpful in intracerebral hemorrhage or edema patients, but detrimental in post-cardiac arrest since ICP goals are different.
- The response to hyperventilation, though, is only temporary and can have a significant rebound.
- A ventricular drain can be used to measure intracranial pressure (ICP) over time.
Mean Arterial Pressure (MAP)
- The ideal range is variable, but typically 60-150 mmHg
- MAP = DBP + 1/3 (SBP – DBP)
- (Systolic Blood Pressure = SBP, Diastolic Blood Pressure = DBP)
Cerebral Perfusion Pressure (CPP)
- CPP should be >70 mmHg ideally, with a lower limit of 50 mmHg.
- CPP = MAP – ICP
Forms of Brain Edema
Vasogenic edema
- Extracellular edema.
- Damage to the blood-brain barrier causes fluid extravasation out of the intravascular space.
- Examples include tumors
Cytotoxic edema
- Intracellular damage
- Due to damage to the cellular membrane itself, such as with an ischemic stroke.
Interstitial Edema
- Increase in brain fluid due to blockage of CSF flow. An example is obstructive hydrocephalus.
Forms of Herniation

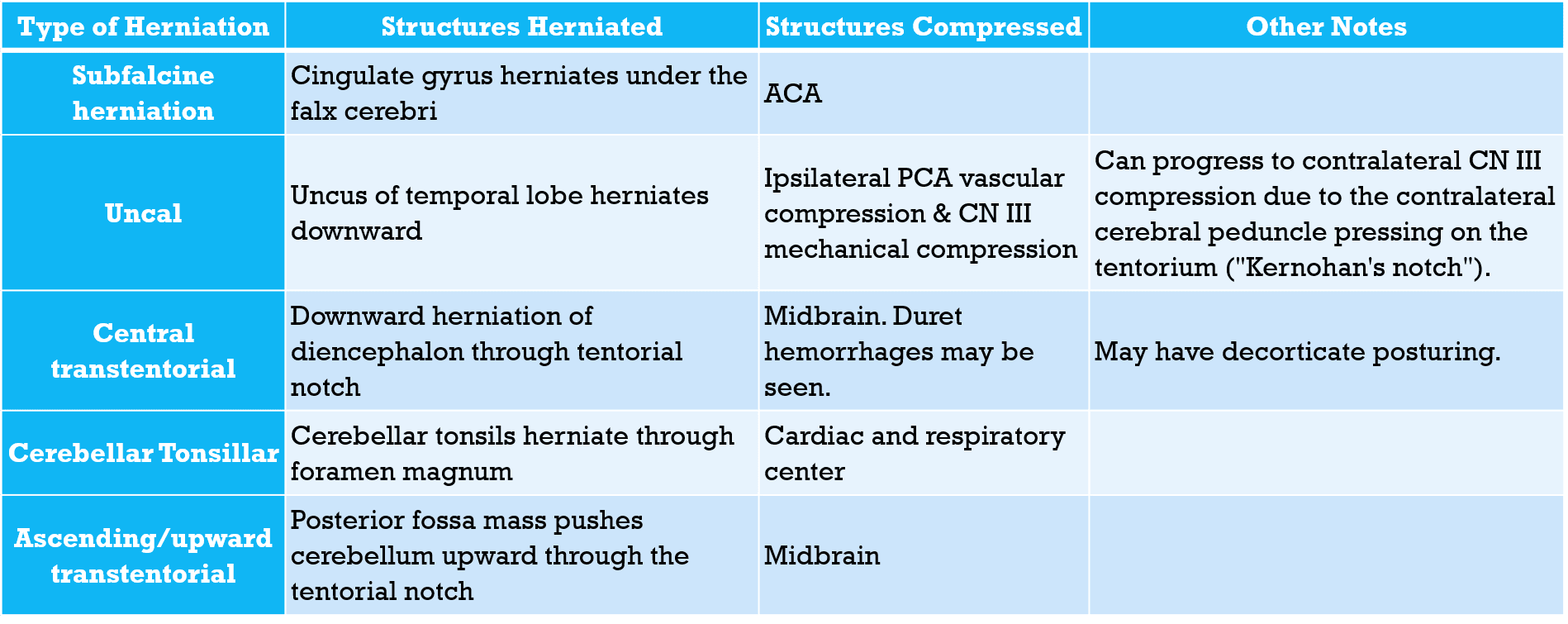

Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
