


Stroke subtypes (by TOAST criteria)
Large-artery atherosclerosis
- The most common cause of ischemic stroke in the world.
- Patients will have either significant stenosis or occlusion of a major brain artery or branch cortical artery.
- Symptomatic Carotid: Stenosis of the common carotid ipsilateral to a TIA or infarct.
- Carotid endarterectomy (CEA) or carotid artery stent (CAS) is indicated if the stenosis is 50-99% in men or 70-99% in women.
- Asymptomatic carotid stenosis should be treated surgically if the stenosis is 80-99%.
- CEA has a higher risk of periprocedural myocardial infarction
- CAS has a higher risk of periprocedural stroke
- Treatment with CEA or CAS can lead to cerebral hyperfusion syndrome, which presents with headaches, visual disturbances, and seizures.
- Occurs secondary to dysautoregulation of cerebral vessels in regions which been in chronic low-flow states.

Atherosclerosis
Atherosclerosis (yellow-white plaques) of the basilar and vertebral arteries.

Thrombus in Atherosclerotic Basilar
A recent thrombus is shown occluding this stenotic atherosclerotic basilar artery.
Cardioembolism
- The most common cause of ischemic stroke in the United States.
- Patients can present similarly with comparable imaging to those with large-artery atherosclerosis but will have a cardiac source for the embolic phenomenon.
- Sources of cardioembolism: Atrial fibrillation, mechanical heart prosthetic valve, left atrial or ventricular thrombus, recent myocardial infarction, dilated cardiomyopathy, valvular heart disease, structural heart defects, tumors, etc.


Lipohyalinosis/small-vessel disease
- Commonly occurs in the lenticulostriate vessels of deep cortical structure.
- Also known as lacunar strokes, these are felt to be related to chronic hypertension, diabetes, and smoking.

Stroke of Other Determined Etiology
Hypercoagulability and coagulopathy
- Examples: Factor V Leiden, antiphospholipid antibody syndrome, protein S/C deficiency, prothrombin gene mutation, antithrombin III syndrome, sickle cell disease, thrombotic thrombocytopenic purpura (TTP), polycythemia, hyperhomocysteinemia, MTHFR gene mutations, and malignancy.
- Blood transfusions can decrease the risk of stroke in patients with sickle cell disease.
- More likely to cause venous events than arterial.
- Examples: Factor V Leiden, antiphospholipid antibody syndrome, protein S/C deficiency, prothrombin gene mutation, antithrombin III syndrome, sickle cell disease, thrombotic thrombocytopenic purpura (TTP), polycythemia, hyperhomocysteinemia, MTHFR gene mutations, and malignancy.
Central nervous system (CNS) vasculitis
- CNS vasculitis is a syndrome caused by a diverse spectrum of diseases that typically involves the gray/white matter junction.
- Diffusion-weighted sequences on MRI will show multiple small focal areas of acute infarction in multiple vascular territories.
- Vessel imaging will show marked beading and segmentation alongside numerous arterial structures.

Primary CNS Vasculitis

- Primary angiitis of the CNS (PACNS):
- Vasculitis confined only to the small-medium sized blood vessels in the brain, spinal cord, and meninges.
- Primary angiitis of the CNS (PACNS):
Moyamoya disease
- Congenital Moyamoya disease is seen most often in patients of Asian descent.
- Mysterin/RNF213 as a susceptibility gene for congenital moyamoya.
- Secondary causes of Moyamoya disease include head/neck radiation, sickle cell disease, neurofibromatosis, and prothrombotic disorders.
- Angiogram will show an abnormal vascular pattern of small net-like lenticulostriate vessels characterized as a “puff of smoke” with severe stenosis or occlusion of the distal internal carotid arteries.

Moyamoya Disease - Pathology:
- Large vessel thickening of the intima, small overgrown dilated small arteries, and regions of ischemic and/or hemorrhagic infarct.
- Congenital Moyamoya disease is seen most often in patients of Asian descent.
Arterial dissection
- Dissections are due to a tear of the vessel wall intima leading to a formation of a false lumen.
- Symptoms can include head/neck pain and Horner syndrome. Ischemic events occur due to thromboemboli formation and less often cerebral hypoperfusion.
- A common cause of stroke in the young. Should be considered in a patient with a history of neck trauma, chiropractic neck manipulation/high-velocity neck injury, or connective tissue disease (fibromuscular dysplasia, Marfan syndrome, Ehlers-Danlos syndrome).
- Dissections are often extracranial and vessel imaging may show a “string sign” or flame-shaped occlusion in the area of the dissection.

Right ICA Dissection
Patent foramen ovale (PFO)
- Seen in roughly 20% of people and its presence alone is not a strong risk factor for ischemic stroke. PFO’s shouldn’t be considered as an etiology for stroke unless a patient presents with a cryptogenic embolic stroke.
- Lesions that are large, have a significant right to left shunt or are accompanied by an atrial septal aneurysm have a higher risk of recurrent stroke.
- While the standard of care for secondary stroke prevention in those with PFO is antiplatelet therapy, recent data suggest that surgical PFO closure for those with high-risk features reduces the risk of recurrent stroke, and should be considered if the patient is <60 years of age.
- PFO closure in young stroke patients decreases the risk of secondary stroke.
- Seen in roughly 20% of people and its presence alone is not a strong risk factor for ischemic stroke. PFO’s shouldn’t be considered as an etiology for stroke unless a patient presents with a cryptogenic embolic stroke.
Air embolus
- The entry of air into the vasculature can be related to surgery, trauma, intravascular catheters, and barotrauma.
- If CTH is performed promptly after insult, air can be seen within the cerebral vessels.
- Treatment includes emergent use of a hyperbaric oxygen chamber, but the prognosis is often poor.
Fat embolism syndrome (FES)
- FES occurs secondary to long bone or pelvic fractures leading to the release of fatty bone marrow into the systemic circulation.
- Emboli obstruct pulmonary arteries leading to respiratory distress. Microemboli can pass through the pulmonary circulatory system and extend into the systemic arterial system and brain leading to small, randomly distributed ischemic strokes.
Hypoperfusion
- Hypoperfusion can cause watershed regions between major vascular territories to become ischemic.
- Imaging will show ischemia along border zone regions of the ACA-MCA and MCA-PCA territories.
- Bilateral ACA-MCA border zone infarcts can cause “man in the barrel” syndrome: upper extremity paralysis with retained strength in lower extremities.
- Bilateral MCA-PCA border zone infarcts can cause Balint’s syndrome: the triad of simultagnosia, oculomotor apraxia, and optic ataxia.

Border zone Infarcts
Mitochondrial Encephalopathy, Lactic Acidosis, and Stroke-like episodes (MELAS)
- MELAS is a mitochondrial disease caused by a mitochondrial DNA mutation to the gene MT-TL1.
- Symptoms of ischemic strokes, seizures, and headaches present before the age of 40.
- Diagnostic testing will reveal elevated cerebral spinal fluid lactate levels, serum lactic acidosis, and ragged red fibers on muscle biopsy
Trauma
Drugs/Toxins
- Common drugs that induce stroke include cocaine and amphetamines.
Stroke of Undetermined Etiology
- A diagnosis that is given to patients in which a cause of a stroke cannot be determined with any degree of confidence.
- Many patients with stroke of undetermined etiology will ultimately be found to have paroxysmal atrial fibrillation with prolonged heart monitoring.



Pathology of Ischemic Stroke
- Brain ischemia leads to excessive extracellular glutamate. This leads to hyperexcitation of neurons and activation of an apoptotic cascade that leads to cell death.
- Gross pathology
- Acutely a gross examination will reveal swelling with effacement of the gray-white junction, and cracking at the interface between the intact and infarcted brain tissue. Over time infarcted tissue becomes sharply demarcated and is eventually replaced by a cavity.
 Acute Infarct with Focal IschemiaDusky discoloration and encephalomalacia are present in the left cerebral hemisphere corresponding to the region supplied by the left internal carotid artery.Remote ACA infarctRemote infarct weeks to months after the initial injury. There are cystic changes with irregular gray-tan cavities. The bordering parenchyma has slight orange discoloration due to the presence of hemosiderin. These cystic changes can be seen in the ACA vascular territory.
Acute Infarct with Focal IschemiaDusky discoloration and encephalomalacia are present in the left cerebral hemisphere corresponding to the region supplied by the left internal carotid artery.Remote ACA infarctRemote infarct weeks to months after the initial injury. There are cystic changes with irregular gray-tan cavities. The bordering parenchyma has slight orange discoloration due to the presence of hemosiderin. These cystic changes can be seen in the ACA vascular territory.
- Acutely a gross examination will reveal swelling with effacement of the gray-white junction, and cracking at the interface between the intact and infarcted brain tissue. Over time infarcted tissue becomes sharply demarcated and is eventually replaced by a cavity.
- Micropathology
- There will initially be no changes on H&E stain for the first 8 hours.
- In the following days, hypereosinophilic anoxic neurons, also known as “red dead neurons,” develop.
- In the following weeks, the lesion undergoes liquefaction as macrophages enter the space and ingest necrotic tissue.
- Thereafter, astrocytes will form a glial scar around the infarct. This is completed in the proceeding months after an ischemic insult.
36 Hours Post Cerebral InfarctNote the numerous macrophages.Gliosis after Remote Infarct




Intraparenchymal hemorrhage
Causes
Trauma
- Parenchymal contusions are a form of traumatic brain injury where multiple microhemorrhages are found on the interface between brain and bone.
- Coup contusions occur beneath the site of impact
- Countercoup contusions occur on the opposite side of the site of impact.
- Patients will often have a concurrent skull or maxillofacial fracture.
- Racoon eyes: Periorbital ecchymoses suggests a fracture of the orbital plate
- Battle sign: Retromastoid ecchymosis suggests a fracture of the petrous portion of the temporal bone.
- Leakage of CSF into the middle ear (CSF otorrhea) or sinus (CSF rhinorrhea) can occur. Samples of leaking fluid can be sent to the lab and tested with beta-2 transferrin assay to distinguish CSF from mucus.

Acute Brain Contusion

Contrecoup Contusion

Old Inferior Frontal Lobe Contusions

Cerebral Contusion
Axial CT head.
Hypertension
- The most common cause of non-traumatic IPH. High blood pressure leads to the rupture of small brittle blood vessels.
- Lesions are located in deep cortical matter and brainstem.
 Hypertensive Pontine HemorrhageCT scan, axial cut.Intracerebral Hemorrhage of Right ThalamusAxial CT. This was secondary to hypertension. Note the intraventricular spread.Intracerebral Hemorrhage of Right Putamen Secondary to HypertensionCT axial cut.Intracerebral Hemorrhage of Left ThalamusThis was secondary to hypertension. Note the intraventricular spread.Right Lentiform Nucleus Hemorrhage secondary to hypertension.Left: Axial CT. Right: Axial MRI GRE.
Hypertensive Pontine HemorrhageCT scan, axial cut.Intracerebral Hemorrhage of Right ThalamusAxial CT. This was secondary to hypertension. Note the intraventricular spread.Intracerebral Hemorrhage of Right Putamen Secondary to HypertensionCT axial cut.Intracerebral Hemorrhage of Left ThalamusThis was secondary to hypertension. Note the intraventricular spread.Right Lentiform Nucleus Hemorrhage secondary to hypertension.Left: Axial CT. Right: Axial MRI GRE.
Cerebral amyloid angiopathy (CAA)
- The second most common cause of non-traumatic brain hemorrhage. Typically presents over the age of 60 with superficial lobar hemorrhages and cortical superficial siderosis.
- Patients are also at risk of TIA-like attacks called “amyloid spells” also known as transient focal neurologic episodes (TFNEs). They are felt to be secondary to cortical irritation from blood products.
- Can be differentiated from typical TIA based on blood products seen on neuroimaging.
- Patients with Alzheimer’s disease are more likely to have CAA.
- MRI will show multiple small silent cerebral microhemorrhages.

Cerebral Amyloid Angiopathy - Pathology will show congophilic waxy pink material (amyloid) in cortical and leptomeningeal arteries with apple-green birefringence.
Vascular malformations
- Arteriovenous malformation (AVM):
- Most likely vascular lesion to cause catastrophic morbidity/mortality.
- Characterized by large abnormal arteries with surrounding thick-walled “arterialized” veins due to high intraluminal pressures.
- Lesions are best appreciated with an angiogram.
- Pathology will show arteries with fragmentation and reduplication of the elastic layer and thick-walled veins with a thin elastic layer.
- While intraparenchymal bleeds are more common, superficial lesions may bleed into the subarachnoid space.
- Gallery of radiographic images and pathology slides of AVMs:
") Right Arteriovenous Malformation (AVM)Left: Axial T2 FLAIR MRI. Right: MRA.Right Arteriovenous Malformation (AVM)T2 brain MRI, axial cut.Left AVMLeft: Axial MRI, T2. Middle: T2 FLAIR. Right: GRE.Left Arteriovenous Malformation (AVM)Left: MRA. Right: Cerebral angiogram.Left Arteriovenous Malformation (AVM)Left: Axial T2 FLAIR MRI. Right: MRA.Vein of Galen MalformationLeft: MRA with AVM. Right: CXR with cardiomegaly.Arteriovenous MalformationNote the tangled mass of vessels in the right occipital cortex.Arteriovenous MalformationNote the arterialization of veins in this section.Arteriovenous MalformationLow power view H&E stain with closely juxtaposed, large-caliber blood vessels with arterialized veins.
Right Arteriovenous Malformation (AVM)Left: Axial T2 FLAIR MRI. Right: MRA.Right Arteriovenous Malformation (AVM)T2 brain MRI, axial cut.Left AVMLeft: Axial MRI, T2. Middle: T2 FLAIR. Right: GRE.Left Arteriovenous Malformation (AVM)Left: MRA. Right: Cerebral angiogram.Left Arteriovenous Malformation (AVM)Left: Axial T2 FLAIR MRI. Right: MRA.Vein of Galen MalformationLeft: MRA with AVM. Right: CXR with cardiomegaly.Arteriovenous MalformationNote the tangled mass of vessels in the right occipital cortex.Arteriovenous MalformationNote the arterialization of veins in this section.Arteriovenous MalformationLow power view H&E stain with closely juxtaposed, large-caliber blood vessels with arterialized veins.
- Cavernous malformation (CM):
- Also called cavernous hemangiomas or cavernomas.
- Much less likely to cause catastrophic bleeding when compared to AVMs.
- Commonly seen in young adults and can be either sporadic or familial.
- CCM1 on chromosome 7q causes familial CMs in those with Hispanic heritage.
- Symptoms include focal neurologic deficits secondary to hemorrhage or seizure.
- If there is an associated developmental venous anomaly (DVA) there is a higher risk of hemorrhage.
- Imaging will show an irregular partially calcified mass with a “popcorn appearance.”
- Pathology will show dilated, closely juxtaposed, thin-walled capillaries and a ring of hemosiderin consistent with remote microhemorrhages.
- Arteriovenous malformation (AVM):






")
")

")
")





Multiple Cavernous Malformations
Axial T2 FLAIR MRI brain with classic “popcorn” appearance.

Left Thalamic Cavernous Malformation
T1 MRI with a hyperintensity that has a “popcorn” appearance. Left: Sagittal view. Right: Axial view.

Left Cavernous Malformation
Left: Axial MRI, T1. Middle: T2 FLAIR. Right: GRE.

Cavernous Malformation located in the left thamaus
CT scan, axial cut.

Acute Hemorrhage in Pontine Cavernous Malformation
Axial T2 FLAIR MRI.

Cavernous Malformation
Trichrome stain showing packed vascular sinuses.
- Charcot-Bouchard aneurysms:
- Associated with chronic hypertension, these lesions are located on small lenticulostriate arteries.
- Rupture leads to deep cortical intraparenchymal bleeds.
- Charcot-Bouchard aneurysms:
Brain tumor
- Atypical IPHs and/or patients with a history of cancer should have an MRI of the brain with and without contrast to evaluate for tumor.
- Metastatic tumors that are likely to bleed include melanoma, renal cell carcinoma > choriocarcinoma, thyroid (papillary) carcinoma > lung, and breast.
- Glioblastomas are highly vascularized primary CNS tumors that can bleed.
- See Tumors and Cysts for more information!
CNS infection (i.e herpes encephalitis)
- Tends to occur in the temporal lobes. See Neuroinfectious Disease for more.
Other
- Hemorrhagic conversion of an ischemic stroke
- Venous infarct
- Vasculitis
- Coagulopathy
- Anticoagulants
Treatment
- Blood pressure regulation (SBP 140-160)
- Reversal of anticoagulation
- If intracranial bleeding occurs with warfarin/NOAC use, treatment can be restarted ~7 to 30 days after the injury if the patient is at high risk for ischemic stroke based on the CHA2DS2VASc score.
- Consideration for surgical intervention if a vascular malformation is found
Subarachnoid Hemorrhage (SAH)
- Patients will present with the complaint of a thunderclap headache or “worst headache of my life”.
- Thunderclap headache means the maximum intensity of the headache is reached in just seconds.
- Other symptoms include nausea/vomiting, meningismus, or syncope at symptom onset.
- SAH can be appreciated on CT but it is not as sensitive as lumbar puncture (LP) in an acute setting.
- LP should be considered in patients when suspicion for SAH is high but the CTH was negative.
- Vasospasm is a serious complication that can cause multifocal infarctions or diffuse hypoxia/ischemia.
- Typically occurs between the 4th and 14th day after hemorrhage, and may present with new focal neurologic deficits and drowsiness.
- The oral calcium channel blocker nimodipine after SAH has been associated with better patient outcomes.
Causes
Ruptured saccular/berry aneurysm
- Hemodynamic stress in high blood flow junctions leads to a breakdown of the elastic lamina and eventual vessel outpouching and aneurysmal development.
- Saccular aneurysms tend to be asymptomatic until they rupture, and are the most common and morbid cause of SAH.
- 85% are located in the anterior circulation (Anterior communication artery, Posterior communicating artery, or bifurcation of MCA)
- Posterior communicating artery aneurysms can cause compression of CN III leading to extraocular movement dysfunction and mydriasis secondary to dysfunction of superficial parasympathetic fibers.
- Posterior circulation saccular aneurysms are found at the tip of the basilar artery.
Fusiform aneurysms
- More common in posterior circulation vasculature.
- Lesions are characterized as a dilation of the entire blood vessel and are less likely to rupture than berry aneurysms.
Mycotic aneurysms
- Secondary septic emboli from endocarditis.
- Lesions are found in the distal branches of intracranial vessels and are best seen on angiography.
- The middle cerebral artery is most commonly affected.
Non-aneurysmal causes of SAH
- Intracranial artery dissection, AVM, trauma, bleeding disorders, drugs, sickle cell disease, etc.
- Gallery of radiographic images and pathology slides of SAH:
Subarachnoid HemorrhageLeft: Normal axial CT. Right: CT with subarachnoid hemorrhage.Subarachnoid Hemorrhage with Intraventricular SpreadAxial CT head. Note the blood pooling in the ventricles.Subarachnoid Hemorrhage from ACA AneurysmLeft: CT scan, axial cut. Right: Cerebral angiogram.Left MCA Aneurysm RuptureCT scan, axial cut.Subarachnoid Hemorrhage in the Circle of WillisCaused by a ruptured berry aneurysm.
Superficial siderosis
- Chronic, slow, and intermittent SAH can lead to superficial siderosis. This is when there is chronic hemosiderin deposition of the brainstem, cerebellum, and cranial nerves leading to gliosis, neuronal apoptosis, and demyelination.
- Symptoms include sensorineural hearing loss, cerebellar dysfunction, dementia, and pyramidal signs.
- Imaging will show a widening of the cerebellar folia with atrophy and hemosiderin deposition.
- Chronic, slow, and intermittent SAH can lead to superficial siderosis. This is when there is chronic hemosiderin deposition of the brainstem, cerebellum, and cranial nerves leading to gliosis, neuronal apoptosis, and demyelination.





Subdural hematoma (SDH)
- Due to the tearing of the bridging veins from minor trauma, SDH is recognized as a blood collection between the dura and arachnoid space.
- Elderly patients are at a higher risk due to brain atrophy.
- CT head will show extra-axial, hyperdense (acute) or iso/hypodense (chronic), crescent-shaped blood that can cross suture lines but can not cross the falx cerebri or tentorium cerebelli.
 Chronic Left Subdural HematomaAxial CT. Note the crescent-shaped lesion is hypodense due to chronicity.Acute Right Subdural HematomaCT scan, axial cut.Acute Subdural HematomaSagittal view.
Chronic Left Subdural HematomaAxial CT. Note the crescent-shaped lesion is hypodense due to chronicity.Acute Right Subdural HematomaCT scan, axial cut.Acute Subdural HematomaSagittal view.



Epidural hematoma (EDH)
- Due to tearing of the middle meningeal artery caused by trauma/temporal bone fracture, EDH is recognized as a blood collection between the skull and dura.
- CTH will show a biconvex shaped hyperdense extra-axial lesion that does not cross suture lines.

Right Epidural Hematoma - Patients will usually have a history of recent head trauma with an initial asymptomatic period before a neurological decline (lucid interval).

- Presenting signs/symptoms are non-specific and can include headache, seizures, decreased level of consciousness, nausea/vomiting, and papilledema and/or vision changes secondary to elevated intracranial blood pressures.
- Severe thrombosis can lead to hemorrhagic and less often ischemic strokes.
- Causes: Oral contraceptives, dehydration, hypercoagulable states, infection (meningitis, ENT infections), malignancy.
- Ear infections have been associated with transverse sinus thrombosis.
- Imaging:
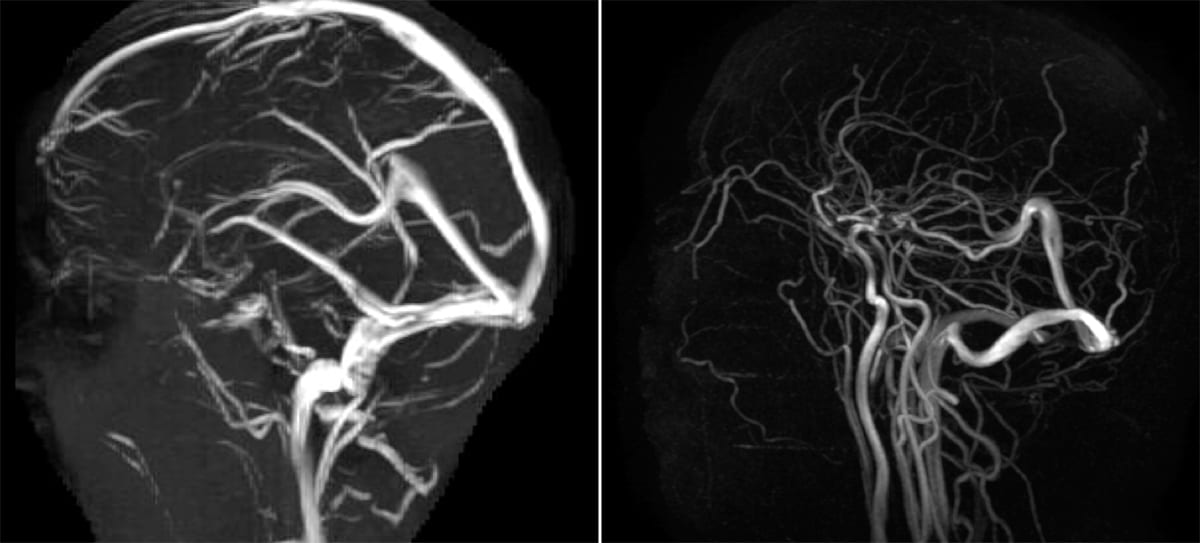
- CTV or MRV is the imaging of choice, which would show a filling defect in the venous system.

Superior Sagittal Sinus Thrombosis - Digital subtraction angiography is the gold standard, but not often required.
- CTH can show deep symmetric cortical hypodensities secondary to vasogenic edema.
- CTV or MRV is the imaging of choice, which would show a filling defect in the venous system.
- Management: Heparin drip and aggressive IV fluid hydration. Endovascular therapy has unclear utility but is sometimes used in patients with seizures and/or severe neurologic deficits.
- Can present secondary to cardiac arrest, drug overdose, drowning, etc.
- If severe HIE, CT head will show generalized edema and loss of cortical sulcation while MRI will show diffuse restricted diffusion of the cortex and deep grey matter.
Hypoxic Ischemic EncephalopathyLeft: Axial DWI. Right: Axial ADC. Diffuse diffusion restriction is present.Hypoxic Ischemic EncephalopathyLeft: Axial MRI, DWI sequence. Right: T2 FLAIR. Shows diffuse hyperintensity indicating diffuse hypoxic injury, secondary to cardiac arrest.Diffuse Hypoxic Damage after Cardiac ArrestAxial CT with diffuse edema and loss of grey-white differentiation. - EEG can have variable patterns
- Favorable prognostic EEG findings are variability, reactivity to external stimuli, sleep patterns, and an increase in background frequencies.
- Poor prognostic EEG findings are burst suppression, monorhythmic patterns, alpha coma (unless in the setting of reversible cause for coma such as metabolic dysfunction, sedative drugs, etc.), generalized periodic discharges, and electrocerebral inactivity (ECI) defined as no EEG activity over 2 microvolts.



Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
