

- Clinical correlations:
- If no Wave I is captured on the recording, no conclusions can be made regarding the auditory pathway.
- When a bilateral auditory stimulus is given (rarely done clinically) in someone with unilateral peripheral hearing loss it will show a unilateral absence of Wave I with an intact ipsilateral Wave V since central auditory pathways are highly crossed.
- Acoustic neuromas can cause a prolonged wave I-III interpeak latency.
- Lesions in the pons can produce abnormalities in waves III, IV, and V.
- Patients with multiple sclerosis are more likely to have an abnormal VEP than an abnormal BAEP or SSEP.
- Prolonged III-V interpeak latency or decreased wave V amplitude can be seen.
- Bilateral absence of all waves except for Wave I after a hypoxic-ischemic injury suggests a poor neurological outcome.

- Clinical correlations:
- Very valuable in monitoring for spinal cord injury in patients undergoing neurosurgical interventions near the spine.
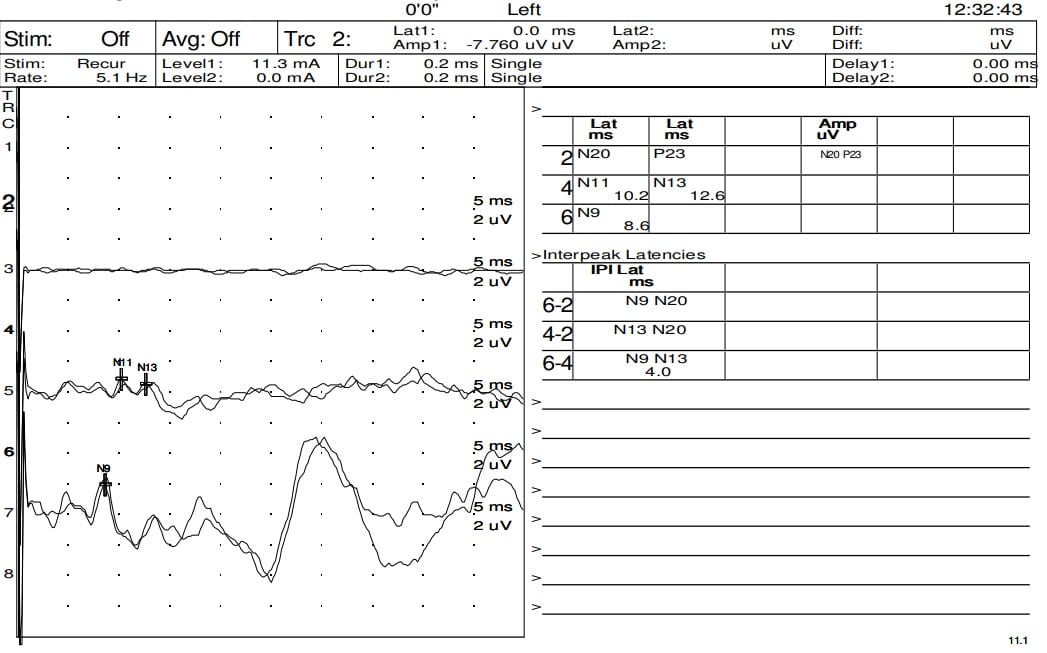
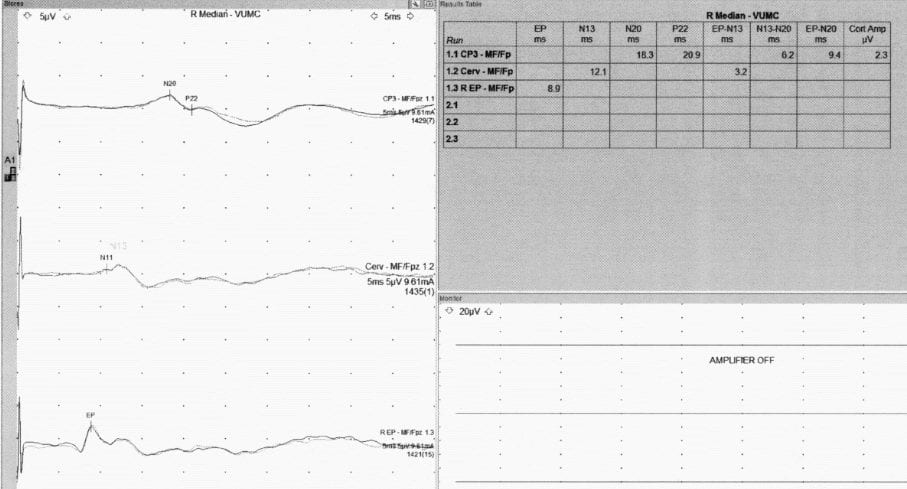
N9 wave is present, but with the absence of brainstem and cortical waves, thus concerning for brain death.
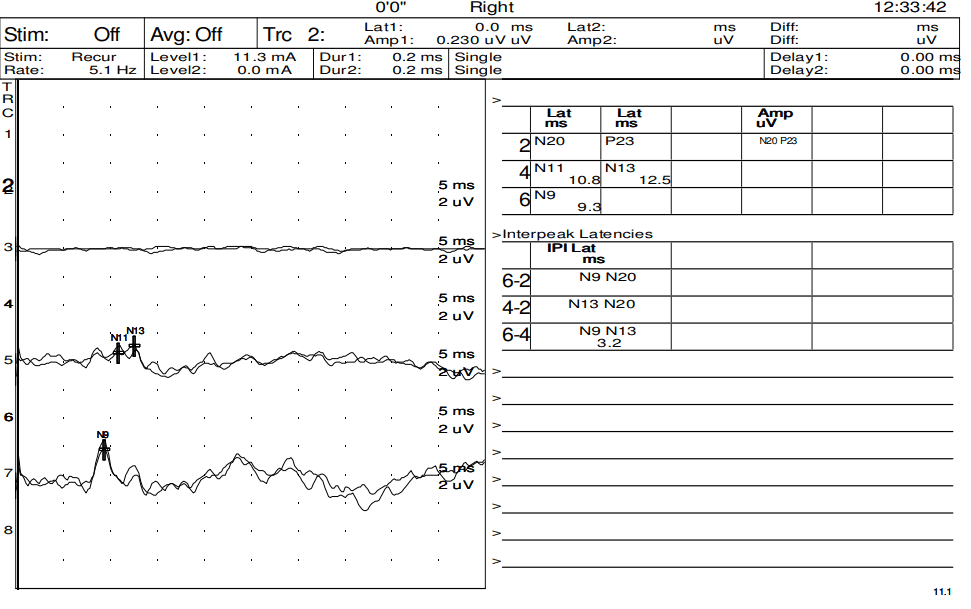
N9 wave is present, but with the absence of brainstem and cortical waves, thus concerning for brain death.
- VEPs can be produced by a flash of a strobe light or visualization of a checkerboard pattern where the boxes shift between black and white. Each eye is stimulated independently so that they can be compared. Patients sit one meter from the monitor.
- The wave of value in VEPs is the P100, which represents occipital cortex stimulation.
- A prolonged P100 latency of a single eye would suggest a pre-chiasmal lesion of the optic pathway (i.e. optic neuritis), especially if the contralateral eye’s P100 latency is normal.
- Hemifield stimulation with large check sizes is required to test post-chiasmal lesions, and even with this technique, only large lesions can be detected.
- If both eyes have prolonged P100 latencies the location of a lesion cannot be localized unless one side is disproportionally more prolonged.
- Poor visual acuity will lead to a decreased P100 amplitude.
- A prolonged P100 latency of a single eye would suggest a pre-chiasmal lesion of the optic pathway (i.e. optic neuritis), especially if the contralateral eye’s P100 latency is normal.
- Clinical correlations:
- Optic neuritis (ON) and multiple sclerosis (MS):
- Very sensitive at detecting optic nerve demyelination secondary to optic neuritis/multiple sclerosis.
- In patients with suspected MS who eventually develop MS, the diagnostic EP abnormalities are 66% for VEPs, 23% for SSEPs, and 13% for BAEPs. Thus, VEPs are superior to other EP modalities in diagnosing MS.
- Abnormal VEPs with prolonged P100 latencies are very typical, even in patients with distant histories of ON who had a complete recovery in visual acuity.
- Patients with ocular blindness will not have appreciable P100 waves.
- Tumor compression of the anterior visual pathways may distort waveforms but doesn’t have a major impact on latency.
- Optic neuritis (ON) and multiple sclerosis (MS):

A normal visual evoked potential of the left eye

Normal visual evoked potential of the left eye
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
