

Tau protein
- Function: Assists in microtubule function as a microtubular associated protein.
- Genetics: encoded by microtubule-associated protein tau (MAPT) gene
- Pathology: Cell death leads to leakage of cellular contents leading to elevated levels of tau and formation of neurofibrillary tangles which are immunoreactive for phosphorylated tau.

Alzheimer’s disease (AD)
- Presents with impairment of memory and at least one other area of cognition.
- Early symptoms include forgetfulness for recent events or newly acquired information, disorientation, and difficulty with complex cognitive functions.
- The degree of memory loss usually correlates with the severity of the loss of cholinergic neurons in the nucleus basalis of Meynert, which has cholinergic projections to the cerebral cortex.
Genetics
- Amyloid precursor protein (APP):
- Located on chromosome 21.
- People with Down syndrome (trisomy 21) have a higher risk of Alzheimer’s disease due to the overproduction of APP.
- Amyloid precursor protein (APP):
- Apolipoprotein E (APOE) gene:
- Susceptibility gene found on chromosome 19.
- Associated with late-onset Alzheimer disease (AD)
- Works by assisting the metabolism and transport of β-amyloid.
- APOE 4 allele increases risk by 5-15 fold.
- APOE 2 allele decreases the risk of AD.
Biomarkers
- Used to help predict conversion from MCI to AD.
- CSF studies: Can be more sensitive than cognitive testing to predict conversion to AD from MCI.
- Elevated total and phosphorylated tau levels due to dying and damaged neurons
- Decreased beta-amyloid 1-42 due to an accumulation of amyloid in plaques.
Pathology
- Microscopic analysis will show extracellular amyloid neuritic plaques and dystrophic neurites with reactive astrocytes and microglia.

Neuritic Plaques
Extracellular amyloid plaque on silver stain, high power.

Alzheimer’s Disease
Amyloid stain with beta-amyloid plaque (low magnification).

Neuritic Plaques
On silver stain.
- Intracellular neurofibrillary tangles, Hirano bodies, neuronal granulovacuolar degeneration, and the deposition of amyloid in the walls of blood vessels can also be seen.
- Neurofibrillary tangles: Flame-shaped intracellular inclusion bodies of phosphorylated tau protein.
- Hirano bodies: Intracellular aggregates of actin and actin-associated proteins, which are not specific to Alzheimer’s disease.
- Granulovacuolar degeneration: Intraneuronal accumulation of large (up to 5 µm diameter) double membrane-bound vacuoles harboring a central granule.

Alzheimer’s Disease
Neurofibrillary tangles on H&E stain.

Granulovacuolar degeneration
High power H&E microscope image showing intraneuronal large vacuoles (arrows), each harboring a central granule. Seen with granulovacuolar degeneration of Alzheimer’s disease.

Granulovacuolar degeneration
Medium power H&E image showing intraneuronal accumulations of large vacuoles harboring a central granule.

Alzheimer’s Disease
Tangles and plaques on lectin stain.

Alzheimer’s Disease
Neurofibrillary tangles on silver stain.

Alzheimer’s Disease
Stain showing a Hirano body.
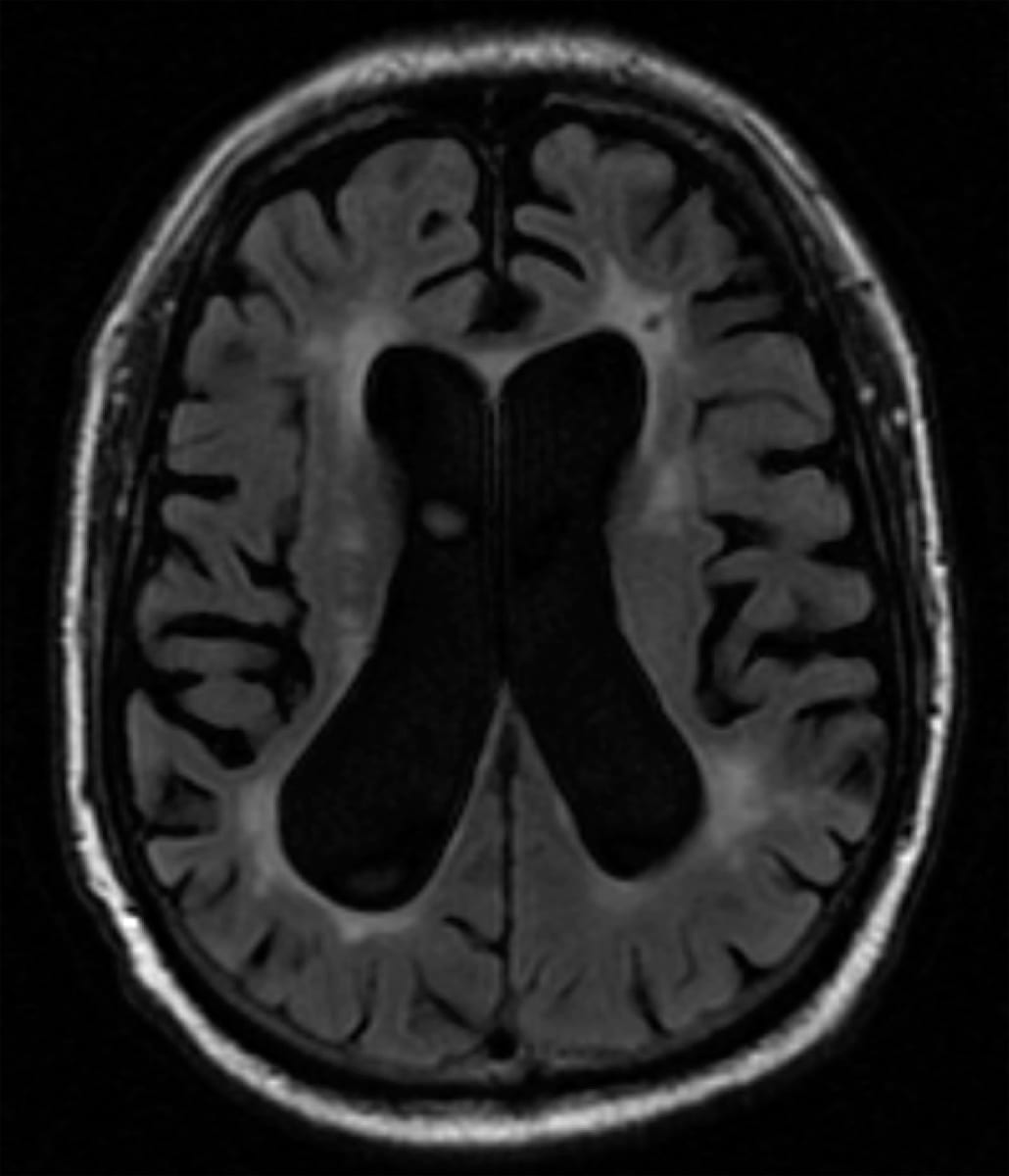
Imaging
- CT/MRI
- Widening of the cortical sulci and enlargement of the lateral ventricles
- Microhemorrhages secondary to amyloid angiopathy can also occur in cortical and subcortical locations.
- Hippocampal and high parietal atrophy

Frontotemporal dementia (FTD)
- Represents a heterogeneous group of disorders with similar behavioral and language dysfunction.
- Presents with language impairment, gait impairments, and behavioral abnormalities including socially inappropriate behavior, apathy, impulsive actions, and compulsive behaviors.
- May also develop nascent artistic abilities.
FTD variants
- FTD with behavioral variant:
- Most common
- Abulia, apathy, poor hygiene, hyperphagia, disinhibition
- Due to involvement of the bilateral anterior temporal lobes, FTD is often associated with Kluver-Bucy syndrome: hyperorality, hypersexuality, and a blunted affect.
- Approximately 15-20% develop concurrent amyotrophic lateral sclerosis (ALS).
- FTD with behavioral variant:
Imaging
- Atrophy of the frontal and temporal lobes (middle and inferior temporal lobes with sparing of the superior temporal gyrus) also known as “knife-edge” atrophy.

Table: PET findings of common neurodegenerative disorders
Condition | PET Scan Findings |
Alzheimer’s Disease (AD) | Hypometabolism in the temporo-parietal cortex, posterior cingulate cortex, and precuneus |
Dementia with Lewy Bodies (DLB) | Hypometabolism in the parieto-occipital cortexes |
Frontotemporal Dementia (FTD) | Hypometabolism in the frontal and anterior temporal lobes
Asymmetric involvement is common, especially in language variants (e.g., primary progressive aphasia) |
Chronic traumatic encephalopathy (CTE)
- Presents in patients with a history of repetitive head impacts (football players, boxers, military, etc.)
- Symptoms include deficits in episodic memory/executive functioning and/or neurobehavioral dysregulation (violent, impulsive, or explosive behavior).
- Pathology: Neurofibrillary tangles of hyperphosphorylated tau within cortical sulci.
Lewy body dementia (LBD)
- It is the second most common dementia after AD.
- Presents with the triad of cognitive decline, symmetric parkinsonism, and visual hallucinations. Other potential clinical features include REM behavior disorder, neuroleptic sensitivity, falls, syncope, and depression.
- REM sleep disorder: Characterized by complex nocturnal behaviors involving vocalizations, hitting, punching, and gesturing.
- Usually, patients with parkinsonian symptoms will partially respond to levodopa but dosing is limited to psychiatric side effects.
- Pathology: Eosinophilic cytoplasmic inclusions composed of alpha-synuclein/Lewy bodies. Spongiform changes in the temporal lobes may also be present.
- Visual hallucinations are associated with high densities of Lewy bodies in the temporal lobes.

Lewy Body

Lewy Body
Alpha-synuclein stain

Lewy Bodies
Medium power microscope slide, positive immunostaining of alpha-synuclein (brown), consistent with an alpha-synucleinopathy.

Lewy Body
Alpha-synuclein stain, high power.
Vascular dementia
- May also be called Binswanger’s disease or multi-infarct dementia.
- Presents with a step-wise cognitive decline with imaging consistent with infarcts and small vessel ischemic disease.
HIV associated dementia
- More often presents in those not on antiretrovirals, but patients can still have some degree of cognitive decline despite HAART therapy.

Prion disease
Creutzfeldt-Jakob disease (CJD)
- Presents with rapidly progressive dementia, cerebellar ataxia, myoclonus, hyperekplexia (exaggerated startle), insomnia, encephalopathy, and ataxia.
- Most presentations are sporadic, and usually presenting between ages 50-70.
- Pathophysiology: There is misfolding of PrP, transforming it from a mainly α-helical structure to a β-pleated-sheet-predominant structure.
- Diagnostic studies:
- MRI will show DWI changes with cortical ribboning, and/or hyperintensity of caudate, putamen, and thalamus.
")
Creutzfeldt-Jakob Disease (CJD)
MRI DWI, axial cut, showing cortical ribboning.
 on DWI MRI")
Creutzfeldt-Jakob disease (CJD) on DWI MRI
Diffusion-weighted axial MRI demonstrates restricted diffusion in the cortical mantle and basal ganglia, characteristic of this disorder.
- Cerebral spinal fluid studies:
- Positive 14-3-3 protein (nonspecific), total tau, and neuron-specific enolase.
- RT-QuIC has the highest sensitivity for the diagnosis of CJD.
- Pathology:
- Spongiform changes, neuronal loss, and gliosis.
- Spongiform changes, neuronal loss, and gliosis.
Variant CJD (vCJD)
- Presents in patients due to the consumption of contaminated beef of those infected with bovine spongiform encephalopathy (BSE).
- Patients usually have a prolonged latency period in comparison to other prion-related diseases.
- Cerebellar dysfunction is typical. Tonsil biopsy is a potential way to diagnose.
- Presents in patients due to the consumption of contaminated beef of those infected with bovine spongiform encephalopathy (BSE).
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
