

Alcohol
- Alcohol’s mechanism of action is not entirely understood, but it acts as an agonist of gamma-aminobutyric acid (GABA, the primary inhibitory neurotransmitter in the CNS) .
- Acute intoxication:
- Presents with slurred speech, incoordination, unsteady gait, and nystagmus.
- Chronic EtOH:
- Can cause vitamin deficiencies such as B12 deficiency and B1 deficiency-related Wernicke’s encephalopathy and Wernicke-Korsakoff disease. See below regarding vitamin deficiencies.
- Subcortical alcohol-related dementia.
- Cerebellar atrophy

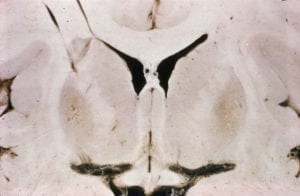
Cerebellar Atrophy
Sagittal section of a cerebellum showing atrophy of the superior part of the vermis secondary to chronic alcoholism.

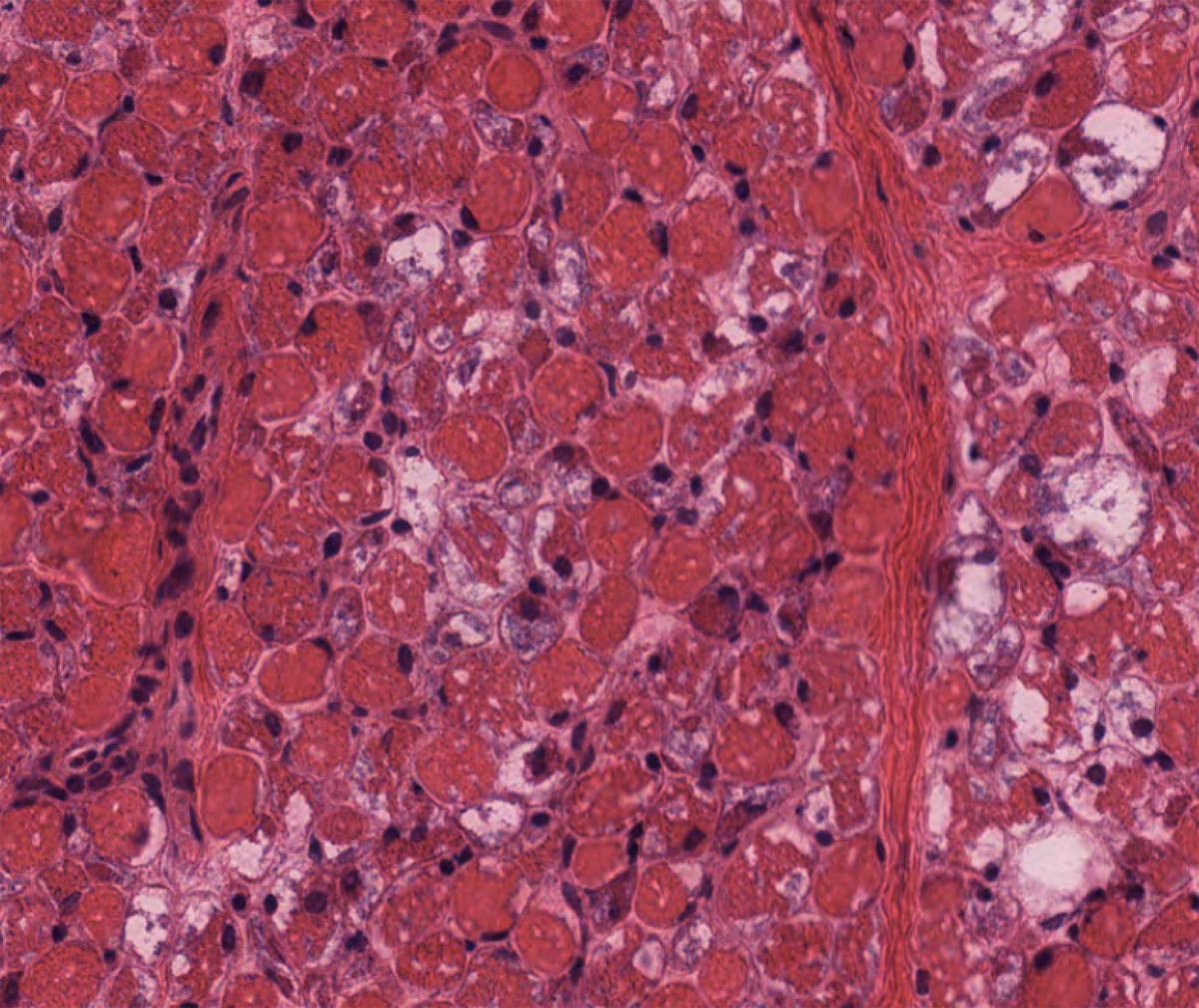
Cerebellar Atrophy
Low power H&E view of cerebellum showing atrophy of the folia from chronic alcoholism.
- Marchiafava-Bignami disease
- Corpus callosum damage.
- Presents with a sudden onset of stupor, coma, and seizures. Can also present with dementia, gait problems, psychiatric disturbances, incontinence, hemiparesis, aphasia, and apraxia of the left hand (due to callosal disconnection).
Methanol
- Ingested as an alcohol substitute and in suicide attempts.
- Methanol → formaldehyde → formic acid.
- Presents with a headache, confusion, hyperventilation and anion gap metabolic acidosis, and visual deficit.
- Pathology: Necrosis and hemorrhage of the putamen and toxic optic neuropathy.
- Treatment: bicarbonate and fomepizole are first-line. Ethanol works similarly to fomepizole. Dialysis may also be needed.
Ethylene Glycol
- Presents with edema and petechial hemorrhages secondary to calcium oxalate deposits within vessels.
PCP
- Presents with nystagmus, hypertension, tachycardia, muscle rigidity, dysarthria, decreased response to pain, and seizures.
Bath salts/methylenedioxypyrovalerone (MDPV)
- Presents with hypertension, tachycardia, delusions, hallucinations, and violent behavior.
Opioids
- Acute overdose will present with miosis (constricted pupils), hypotension, bradycardia, and decreased respirations.
- Can be treated with naloxone.
- Constipation can occur with chronic use.
- Long-term treatment for opioid dependence includes naltrexone (long-acting opioid antagonist), methadone, or buprenorphine.
- Withdrawal symptoms include lacrimation, rhinorrhea, diaphoresis, mydriasis, and yawning.
- Clonidine (alpha 2-receptor agonist) can blunt the sympathetic symptoms associated with opioid withdrawal.
- Meperidine is metabolized into a neurotoxic metabolite that can provoke myoclonus, tremors, and seizures.
Benzodiazepines
- Mechanism: Increases frequency of GABAA channel opening.
- Barbiturates, on the other hand, increase the duration of GABAA opening.
- Most benzodiazepines are metabolized by the cytochrome p450 system.
- Lorazepam, oxazepam, and temazepam, however, undergo direct glucuronidation without cytochrome p450 metabolism and therefore can be used in patients with renal or hepatic dysfunction with only minor effects on pharmacokinetics.
Cocaine
- Works by inhibiting dopamine reuptake and increasing dopamine concentrations in the nucleus accumbens. Also inhibits the reuptake of serotonin and norepinephrine.
- Acute intoxication presents with mydriasis, euphoria, and tachycardia.
Amphetamines
- Amphetamine intoxication presents similarly to cocaine, except the mechanism of action is through both the direct release of dopamine and norepinephrine and the inhibiting of reuptake.
Nitrous Oxide (inhaled)
- Exam: progressive paresthesias secondary to myelopathy of the posterior and lateral columns, mimicking B12 deficiency. Additional symptoms include ataxia, weakness, and positive Lhermitte’s sign.
- Pathophysiology: Irreversible oxidization of methylcobalamin which interferes with the vitamin B12-dependent conversion of homocysteine to methionine as well as methyl-malonyl CoA into succinyl CoA. Homocysteine levels will be elevated. Treat with methionine supplementation.
Glue (Toluene)
- Inhalation of toluene causes myelin damage and diffuse leukoencephalopathy.
“Chasing the Dragon”
- Inhalation of heated heroin or morphine fumes. Can produce a toxic leukoencephalopathy.
Carbon Monoxide
- When inhaled it binds to hemoglobin with 100 times the affinity of oxygen, leading to poor oxygen-carrying capacity.
- Will be seen in patients with wood-burning stoves in the winter or in suicide attempts from motor vehicle fumes.
- Burning homes cause carbon monoxide and cyanide poisoning from burning synthetic polymers (i.e. vinyl couch).
- Treatment: 100% O2 or hyperbaric O2.
- Pathology: Bilateral globus pallidus necrosis and hemorrhage. Gross pathology will show a swollen congested brain with a cherry red color.
- Imaging: T2 hyperintense globus pallidi. The globus pallidus will also have reduced diffusion of DWI sequences.

Carbon Monoxide Poisoning
Bilateral globus pallidus hemorrhage.

Carbon Monoxide Poisoning
Left: T2 FLAIR. Right: DWI. Note the bilateral globus pallidus hyperintensities.
Botulism
- Presents with muscle weakness, ptosis, dysphagia, double/blurred vision, autonomic dysfunction and altered mental status.
- Infants present with hypotonia and characteristic raspy cry.
- Exposure is often through the environment: inhaled spores from the soil.
- Foodborne botulism
- Adults present 18 to 36 hours after eating contaminated food
- Common foods are home-canned goods or honey.
- Wound botulism
- Can occur secondary to parenteral drug use.
- Will present 10-14 days after exposure.
- Pathophysiology: Inhibition of acetylcholine release from the presynaptic neurons due to inhibition of SNARE (soluble NSF attachment protein receptor) proteins.
Organophosphate poisoning
- Presents with pinpoint pupils, excessive salivation, weakness, and respiratory failure in severe cases.
- Often seen in farmers due to insecticide exposure.
- Mechanism of action: aggressive acetylcholinesterase inhibition.
Pantothenate kinase-associated neurodegeneration (PKAN)
- Also called Hallervorden-Spatz disease.
- Presents with dysarthria, spasticity, choreoathetosis, pigmented retinopathy, equinovarus deformity.
- Secondary to pantothenate kinase gene (PANK2), Ch 20p13.
- Pathology: Iron accumulation within the globus pallidum and pars reticularis.
- Radiology: MRI will show an “eye of the tiger sign”; there is a hypointense lesion in the bilateral basal ganglia with a central hyperintensity which represents gliosis.

Pantothenate Kinase Deficiency
Axial MRI, T2 FLAIR, showing increased T2 signal in the bilateral globus pallidi, consistent with iron deposition.

Pantothenate Kinase Deficiency / Hallervorden-Spatz Syndrome
Axial MRI, T2 FLAIR, showing increased T2 signal in the bilateral globus pallidi, consistent with iron deposition.
Acid α-glucosidase deficiency (Pompe disease)
- Also known as glycogen storage disease type II or acid maltase deficiency, this autosomal recessive enzyme deficiency causes glycogen accumulation in lysosomes in organs, especially heart, muscle, and CNS.
- Due to mutations of the GAA gene.
- Infantile Pompe disease: presents in the first few months of life with hypotonia, macroglossia, failure to thrive, and cardiomyopathy.
- Late-onset Pompe disease: variable severity of presentation, usually without cardiomyopathy. Can present from years to decades of life.
- Diagnosis: screening dried blood spots (DBS) and confirmatory GAA mutation genetic analysis.
- Pathology: PAS+ glycogen-filled lysosomes (vacuolar myopathy) on muscle biopsy.
- EMG may show myotonia.
- Treatment: enzyme replacement with alglucosidase alfa.
GLUT-1 deficiency
- Presents with refractory seizures in an infant with developmental delay, microcephaly, hypotonia, spasticity, ataxia, and dystonia.
- Pathophysiology: Mutation in SLC2A1 causes GLUT-1 deficiency, and thus unable to transport glucose into the brain, which results in low CSF glucose, while lactate is low-normal.
- Treatment: Ketogenic diet because it converts brain energy utilization from primarily glucose to an alternative fuel source of ketones.
Galactosemia
- Deficiency of Galactose 1-phosphate uridyl transferase.
- Intellectual disability, cataracts, failure to thrive, increased ICP, cerebral edema. Susceptible to E. coli infections.
- Treatment: eliminate lactose and galactose from the diet.
Urea cycle enzyme deficiencies
- Exam: If partial, adolescent or early adult-onset neuropsychiatric symptoms including episodic psychosis, depression, and bipolar disorder. These attacks frequently accompanied by gastrointestinal symptoms can be precipitated by high protein ingestion, periods of fever, and can be triggered by valproate
- X-linked UCD can present with strokes.
Phenylketonuria (PKU)
- Phenylalanine hydroxylase deficiency → phenylalanine (Phe) and derivatives build up → neuron death.
- Presents with delayed developmental, short stature, intellectual disability, mouse-like musty odor, possible seizures.
- Treatment: Diet restricted in Phe and protein.
Kearns-Sayre syndrome
- Mitochondrial inheritance disorder that presents with the triad of:
- Chronic progressive external ophthalmoplegia
- Retinitis pigmentosa
- Onset before 20 years of age.
- Also can commonly have heart block, short stature, sensorineural hearing loss, cerebellar ataxia and endocrine dysfunction.
- CSF will have elevated protein.
- As with many mitochondrial disorders, may see ragged red fibers on pathology.
Glutaric acidemia type I (GA 1)
- Deficiency of mitochondrial enzyme glutaryl-CoA dehydrogenase activity causes progressive macrocephaly, striatal necrosis, basal ganglia and frontotemporal degeneration.
- Elevated levels of serum GA, 3HGA, tGA.
Methylmalonic acidemia (MMA)
- deficiency of mitochondrial enzyme L-methylmalonyl-CoA mutase activity causes MMA and lactic acid build-up.
- Presents in infancy (after proteins added to diet) with developmental delay, lethargy, hypotonia, hepatomegaly, coma, and sometimes death.
- marked bilateral destruction of the globus pallidus
- Treatment: Low protein diet. Some are responsive to vitamin B12 injections.
Maple syrup urine disease
- Mitochondrial branched-chain α-ketoacid dehydrogenase deficiency →
- accumulation of branched-chain amino acids.
- Newborns with poor feeding, opisthotonic posturing, hypertonia, failure to thrive, and seizures. Urine with maple syrup scent.
- MR spectroscopy with a branched-chain amino acid spike.
Biotinidase deficiency
- Presents with alopecia, skin rash, developmental delay, visual/hearing impairment, and seizures.
- MRI shows hyperintensity in periventricular white matter and atrophy.
- Treatment: responds to high doses of oral biotin (vitamin B7).
X-linked adrenoleukodystrophy (X-linked ALD)
- ABCD1 gene/protein mutation → impaired peroxisomal β-oxidation → accumulation of very-long-chain fatty acids.
- Varied presentation, but affects bilateral white matter of the brain and adrenal glands.
- Most common presentation is either childhood (4–8 years old) or adult form, with rapidly progressive ataxia, spasticity, personality change, visual/auditory deficits, and seizures.
- MRI is strongly suggesting, showing a bilateral posterior to anterior progression of white matter disease.
Zellweger syndrome
- Also known as cerebrohepatorenal syndrome.
- Occurs secondary to peroxisomal dysfunction due to a PEX gene mutation.
- Infantile form presents with hypotonia, craniofacial dysmorphisms, glaucoma, and sensorineural hearing loss.
- Blood work will show elevated very-long-chain fatty acids.
Homocystinuria
- Symptoms include myopia, dislocation of the lens at the front of the eye (lens subluxation), increased risk of blood clotting, osteoporosis, sometimes developmental delay and learning problems.
- Mutation in CBS gene
(cystathione-β-synthase) - Buildup of homocysteine and methionine.
- Treatment: Low protein diet, Vitamin B6, and betaine, folate (B9), and cobalamin (B12).
Wilsons disease
- Copper accumulation due to errors of copper transport. Read more in the Movement Disorders Chapter.
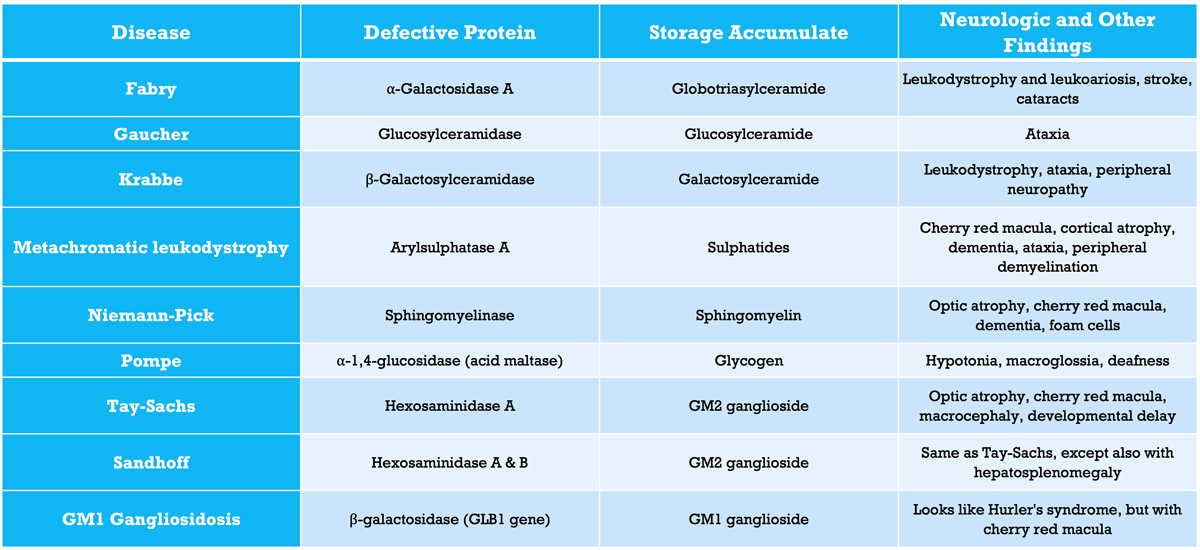
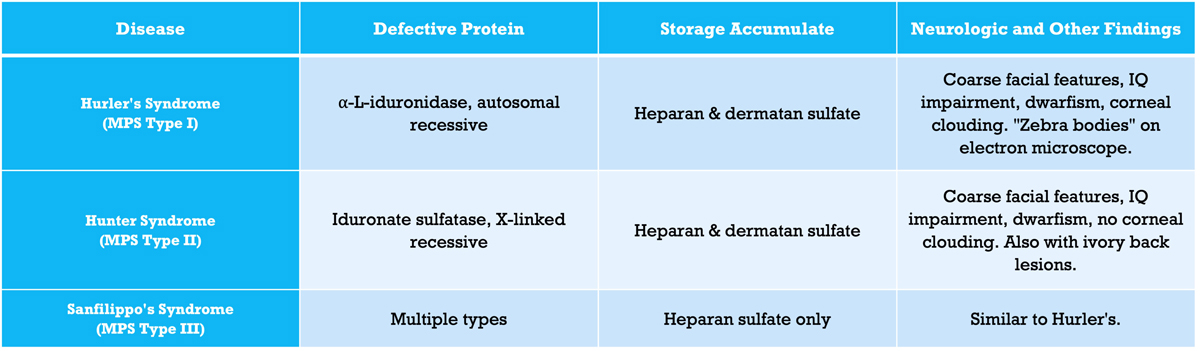
Lysosomal storage disorders
Vitamin A deficiency
- Vitamin A is important for both epithelial cell proliferation and retinal cell function, and thus deficiency can cause keratomalacia and is the leading cause of childhood blindness worldwide.
Vitamin B1 (thiamine) deficiency
- Can cause dry or wet beriberi, Wernicke’s encephalopathy, or Wernicke-Korsakoff syndrome
- Seen in patients with malnourishment (i.e. bariatric surgery, anorexia, alcoholism)
- Dry beriberi: Bilateral peripheral motor and sensory neuropathy with weakness and hyporeflexia. (Wet beriberi is primarily a cardiac disease with cardiac failure).
- Wernicke’s encephalopathy:
- Triad of confusion, ataxia, and nystagmus. Also can have extraocular motility deficiencies.
- Wernicke-Korsakoff Syndrome: Chronic and irreversible progression of mental impairment with short-term memory loss and confabulation.
- Imaging: MRI will show hyperintense signals in the periaqueductal gray area, mammillary bodies, and dorsal medial nucleus of the thalamus.

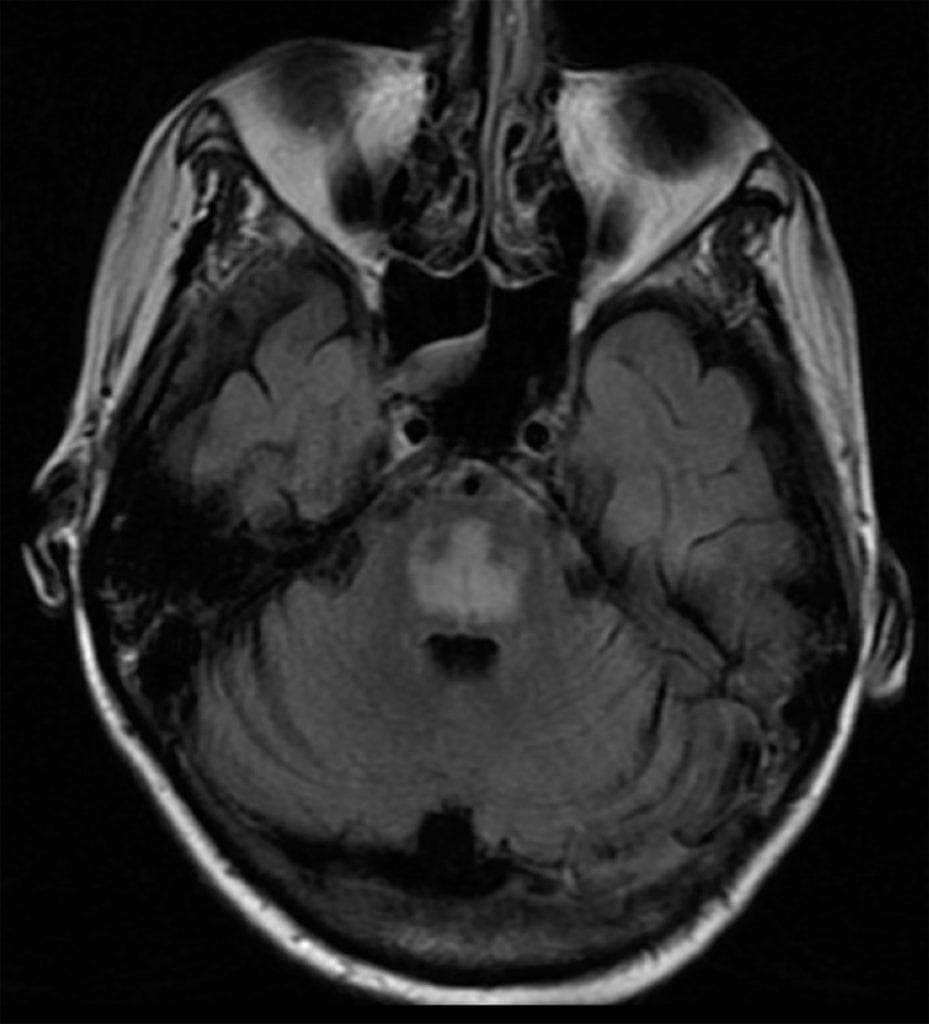
Wernicke’s Encephalopathy
T2 FLAIR hyperintensity of the periaqueductal grey.

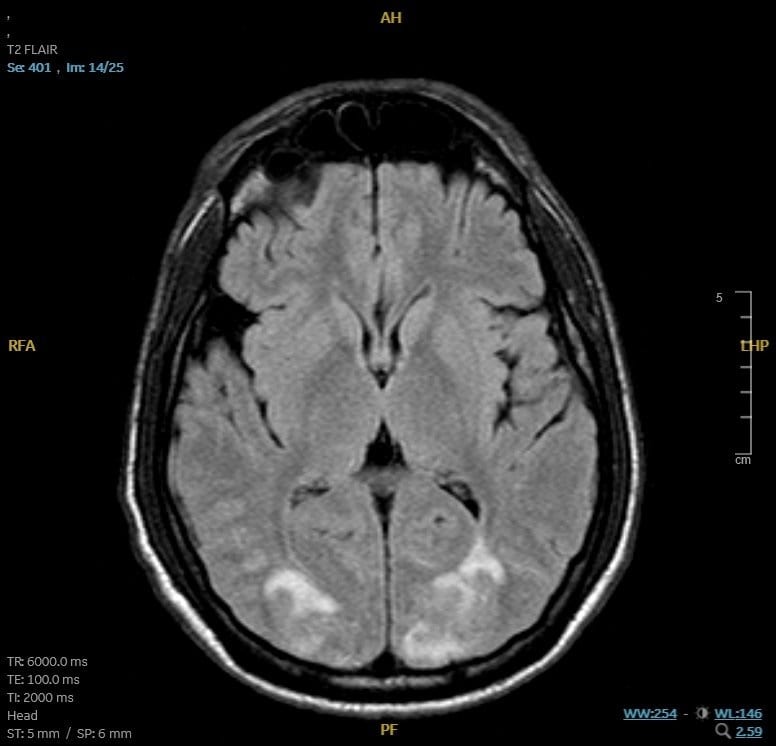
Wernicke’s Encephalopathy
Axial T2 FLAIR MRI showing hyperintensity of the periaqueductal grey and dorsomedial thalamus.
- Treatment: Vitamin B1 replacement.
- If replacing B1 in alcoholics, make sure it is given prior to glucose. Giving glucose before B1 replacement can lead to worsening of Wernicke’s encephalopathy.
Vitamin B3 (Niacin) deficiency
- Causes a disease called pellagra. Occurs as a result of malnutrition or absorption problems.
- Triad: “The 3 D’s” of dementia, dermatitis, and diarrhea. Other neurologic manifestations include peripheral neuropathy and myelopathy.
Vitamin B6 (pyridoxine) deficiency
- Can be caused by long term treatment with the tuberculosis drug Isoniazid.
- Can cause an axonal neuropathy with hyporeflexia and weakness, and/or seizures.
- Vitamin B6 toxicity is rare but can cause a sensory neuronopathy affecting dorsal root and trigeminal ganglia.
Vitamin B9 (folate) deficiency
- During in utero development, causes spina bifida and anencephaly. Folate deficiency in infants can cause irritability, ataxia, psychomotor retardation, and optic neuropathy.
- Recommended daily intake:
- 400 mcg for women of child-bearing age
- 4000 mcg during pregnancy if history of a child with a neural tube defect.
Vitamin B12 (cobalamin) deficiency
- Caused by low intake (vegan diet), pernicious anemia, fish tapeworm (Diphyllobothrium), ileal resection, nitrous oxide abuse, and inflammatory bowel disease.
- The terminal ilium is particularly important for absorption of vitamins B12, A, D, E and K.
- Can cause subacute combined degeneration affecting the posterior columns and lateral corticospinal tracts, evidenced by proprioception deficits.
- Concurrent symptoms: Macrocytic anemia
- Homocysteine and methylmalonic acid may be elevated.
- Treatment: Replete vitamin B12, unless the deficit is caused by nitrous oxide abuse, then use methionine.
Vitamin E deficiency
- Associated with adult-onset cerebellar ataxia.
- Can be seen in patients with cystic fibrosis, Crohn’s disease, short bowel syndrome
- A mutation of the gene encoding for alpha-tocopherol-transfer protein (a-TTP) can also cause Vitamin E deficiency.
- Exam: truncal and limb ataxia, decreased deep tendon reflexes, decreased vibratory and position sense.
Primary CoQ-10 deficiency
- Can produce a myopathy or progressive cerebellar degeneration, reflecting the key role of CoQ-10 as an electron shuttle between complexes I or II and complex III in the electron transport chain.
Copper deficiency
- Presents with myelopathy and polyneuropathy, comparable to subacute combined degeneration from vitamin B12 deficiency.
- Commonly caused by malabsorption disease such as bariatric surgery, overuse of cold prevention supplements, or from zinc toxicity.
- Zinc toxicity: Can be secondary to frequent usage of denture adhesive cream.
- Serum copper and ceruloplasmin will be low if checked.
Zinc deficiency
- Helps regulate GABA and glutamate neurotransmission, and deficiency in utero and early life can cause intellectual disability, tremors, and rash.
Hyponatremia
- Can present with delirium, weakness, and seizures
- Can be seen in marathon runners.
- Rapid correction of sodium can lead to central pontine myelinolysis (CPM).
Hepatic encephalopathy
- Presents in patients with end-stage liver disease due to the accumulation of neurotoxic substances
- Symptoms include altered mental status, asterixis, and in severe cases coma.
- Elevated ammonia levels are seen
- Head imaging may reveal diffuse cerebral edema or T1 hyperintensities in the basal ganglia
- Electroencephalogram may reveal generalized periodic waves with triphasic morphology.
Posterior Reversible Encephalopathy Syndrome (PRES)
- Presents with seizures, altered mental status, vision changes, and focal neurologic symptoms.
- Risk factors include bevacizumab, tacrolimus, cyclosporine, eclampsia, uremia, and extreme hypertension.
- Pathophysiology: Dysfunction of the posterior circulation autoregulation.
- Imaging: Symmetric subcortical/cortical vasogenic edema seen predominantly in the occipital and parietal lobes.
- Treatment: Discontinuing the causal agent and/or treating uncontrolled blood pressure. Patients often have a near-complete recovery.
Fahr disease
- Presents with abnormal calcification within the basal ganglia, and thalamus.
- Symptoms include headache, movement disorders, and seizures.
Log in to View the Remaining 60-90% of Page Content!
Important: If you signed up after 1/1/2026, or if you opted to migrate your old account to the new & improved platform (same great content, better experience), please log in at nowyouknowmed.com
