If you haven’t yet had that late-night call from the emergency department about possible meningitis, trust me, it’s coming. And when it does, you’ll realize that neck pain isn’t just for the patients – it’s shared with residents too! But let’s get serious for a moment: bacterial meningitis is a terrifying infection. Back before 2002, we were unsure whether to include steroids like dexamethasone in the treatment. Then came the study by de Gans and van de Beek, clearing up the confusion. Let’s break down what they found…
This multicenter, prospective, randomized, double-blind, placebo-controlled trial recruited 301 adults diagnosed with bacterial meningitis across various European centers. Participants were randomly assigned to receive either dexamethasone (10 mg every 6 hours for 4 days) before or with the first dose of antibiotics, or placebo. The primary outcome was the score on the Glasgow Outcome Scale, assessed 8 weeks after randomization, with scores of 5 (mild or no disability) considered favorable and 1 to 4 unfavorable. Secondary outcomes included death, specific neurological deficits (e.g., hearing loss), and side effects such as gastrointestinal bleeding and hyperglycemia.
Treatment with dexamethasone significantly reduced unfavorable outcomes from 25% to 15% (RR, 0.59; 95% CI, 0.37 to 0.94; p=0.03) and mortality (RR, 0.48; 95% CI, 0.24 to 0.96 P=0.04). In pneumococcal meningitis mortality and unfavorable outcomes were also reduced. Gastrointestinal bleeding actually occurred less in the dexamethasone group.
The 2002 study by de Gans and van de Beek shaped the future of bacterial meningitis treatment by supporting the use of dexamethasone, citing a reduction in mortality and unfavorable outcomes. A subsequent Cochrane review found dexamethasone to be associated with significantly reduced hearing loss but no difference in overall mortality. In line with the European Society of Clinical Microbiology and Infectious Diseases guidelines and Infectious Disease Society of America’s practice guidelines for the management of bacterial meningitis, current clinical practice requires the prompt administration of dexamethasone as soon as a preliminary diagnosis of bacterial meningitis is suspected, alongside the immediate initiation of empiric antibiotics. Ceftriaxone is preferred, with vancomycin added in North America to fight resistant strains.
Remember that prompt administration of dexamethasone is paramount for the patient! A large systematic review found that a delay of two hours after arrival can result in a twofold increase in mortality and if delayed three hours, a heightened risk of neurological morbidity (OR 1.79, 95% CI 1.03–3.14). Another study revealed that even an hour’s delay can lead to an increase in mortality and morbidity ranging from 13% to 30%. These findings reinforce the urgency and precision required in our clinical response to bacterial meningitis, ensuring the best possible outcomes for our patients.
Hopefully, next time you are called by the Emergency room for someone with neck stiffness and a fever this study will remind you of this important additional component of meningitis patient management!
Feel free to review the original article yourself here!
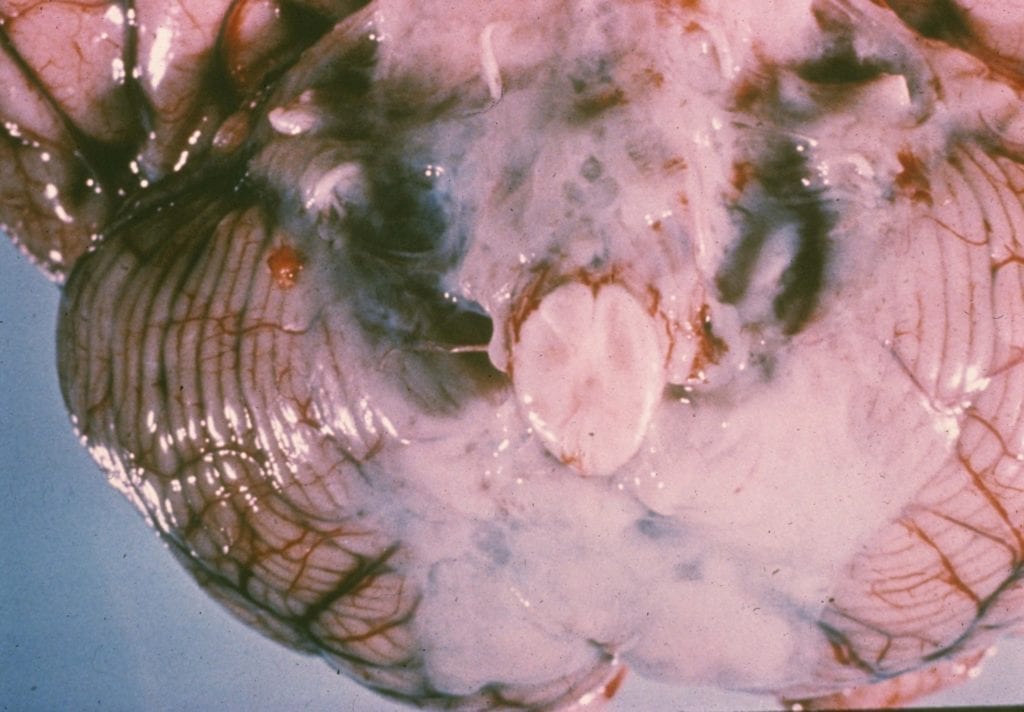
Check out this pathology image of bacterial meningitis from our website below: